
Differentiating between Intestinal Tuberculosis (ITB) and Crohn's Disease
A comprehensive analysis of CT scan findings in the ileocecal region
Key Insights
- Imaging Patterns: Both ITB and Crohn's Disease can show similar mural thickening and lymphadenopathy in the ileocecal region, but subtle differences exist in the nature, extent, and distribution of these changes.
- Characteristic Features: ITB often demonstrates homogeneous smooth mural thickening with minimal fat stranding and discrete lymph nodes, while Crohn's Disease, particularly in its chronic course, may show longer segments of involvement, more prominent fat proliferation, skip lesions, and additional findings such as the comb sign.
- Diagnostic Integration: Accurate differentiation requires correlating CT imaging features with clinical history, laboratory tests, potential biopsy findings, and response to medical therapy.
Introduction
The differentiation between Intestinal Tuberculosis (ITB) and Crohn's Disease (CD) based on CT imaging is a challenging task due to overlapping imaging features. Both conditions commonly involve the terminal ileum, ileocecal junction, and proximal cecum, and they can present with mural thickening, lymphadenopathy, and varying degrees of fat stranding. This detailed analysis will discuss the radiological imaging findings, clinical context, and further diagnostic work-ups necessary for distinguishing between ITB and CD.
Understanding the Imaging Findings
CT Scan Features
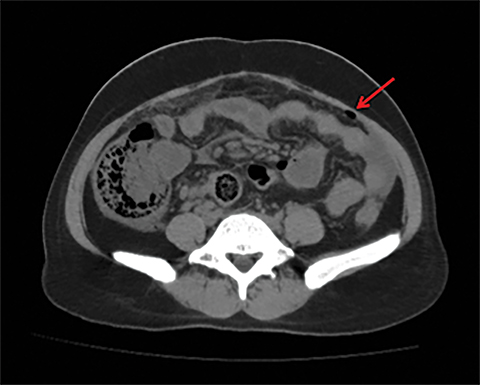
The CT scan study under discussion demonstrated homogeneously enhancing, smooth mural thickening involving the terminal ileum, the ileocecal junction, and the proximal cecum. Alongside this, there is minimal perilesional fat stranding and the presence of homogeneously enhancing, discrete lymph nodes that are up to centimeter-sized in the regional mesentery. Importantly, there is no evidence of any proximal obstruction or abnormal air-fluid levels noted in the bowel loops. Each of these features contributes clues toward a differential diagnosis which is best understood by analyzing them separately.
Mural Thickening
Homogeneous smooth mural thickening is a hallmark finding in both ITB and CD. However, certain nuances help in differentiating between them:
- In ITB, wall thickening is typically smooth and homogeneous, and may often be associated with less pronounced mesenteric fat stranding. The thickening seen in ITB is usually less than 6 mm, reflecting a more subtle inflammatory process.
- In contrast, Crohn's Disease usually presents with longer segments of disease involvement. In chronic CD, asymmetric thickening, “skip lesions,” and transmural inflammation may be observed. Other findings in CD such as the comb sign (indicating prominent vasa recta) and creeping fat may be present, although these may be less obvious in early or mild disease.
Perilesional Fat Stranding
Fat stranding on CT imaging often reflects the degree of inflammation extending into the pericolic or perienteric fat:
- Minimal perilesional fat stranding, as noted in this study, might favor the picture of ITB. In ITB, the inflammatory reaction is usually more localized, and there is less exuberant fat change.
- In Crohn's Disease, particularly in its more active or fulminant stages, there is generally more extensive mesenteric fat proliferation, which can accentuate or mask the inflammatory areas. The increased fat density is a response to chronic inflammation and is often described as "creeping fat."
Lymphadenopathy
The presence and character of lymphadenopathy provide pivotal information in differentiating between ITB and CD:
- ITB is often associated with lymph nodes that are discrete, homogeneously enhancing, and can sometimes show necrosis. Although in the described CT scan, lymph nodes appear homogeneously enhancing up to a centimeter in size without overt necrosis, this feature remains more suggestive of an infectious/inflammatory process such as ITB.
- Conversely, in Crohn's Disease, while lymph nodes can be present, they are usually less defined and not as homogeneously enhancing. Additionally, lymphadenopathy in CD is not typically associated with central necrosis. The absence of necrotic nodes here slightly leans away from ITB, but the overall enhancement pattern still supports an infectious etiology.
Obstruction and Air-Fluid Levels
The absence of proximal bowel obstruction or abnormal air-fluid levels suggests that both conditions are in a phase without significant mechanical complications.
- In Crohn's Disease, chronic inflammatory changes may eventually lead to strictures and subsequent obstruction. The absence of obstruction in the present CT scan implies that if it is CD, the disease might be in its early or mild stage without complications such as strictures or fistula formations.
- In ITB, while intestinal obstruction can occur, particularly in advanced disease owing to fibrotic strictures, the findings here do not demonstrate such early complications.
Comparative Analysis: ITB vs. Crohn's Disease
Distinctive Features on CT
While the CT findings in this study can be consistent with either ITB or CD, several nuances can help in guiding the differential diagnosis. The following table provides a side-by-side comparison of key CT findings in both conditions:
| Feature | Intestinal Tuberculosis (ITB) | Crohn's Disease (CD) |
|---|---|---|
| Mural Thickening | Smooth, homogeneous, usually 6 mm | Asymmetric or focal thickening, generally >6 mm |
| Extent of Involvement | Usually short segment involvement | Often longer segments with skip lesions |
| Fat Stranding | Minimal perilesional fat stranding | Prominent mesenteric fat proliferation and "creeping fat" |
| Lymphadenopathy | Discrete, homogeneously enhancing, potential central necrosis | Less defined, less homogeneously enhancing, rarely necrotic |
| Associated Findings | Generally lacks severe complications like fistulas in early stages | May show comb sign, fistulas, abscesses, and other chronic inflammatory changes |
| Obstruction | Not typically seen in early stages | May progress to strictures and obstruction in chronic cases |
Clinical and Histopathological Correlation
In the context of ambiguous CT findings, it becomes crucial to integrate imaging observations with clinical data and other diagnostic studies:
Clinical History
A thorough clinical history is vital in distinguishing between ITB and Crohn's Disease. Key points include:
- Geographical and Epidemiological Factors: ITB is more prevalent in areas with a high incidence of tuberculosis. A history of exposure to tuberculosis, previous pulmonary TB, or living in endemic areas can tilt the suspicion towards ITB.
- Systemic Symptoms: ITB often presents with systemic features such as fever, night sweats, weight loss, and malaise. Crohn's Disease may present with similar systemic signs but is often associated with a longer history of gastrointestinal symptoms such as chronic diarrhea, abdominal pain, and extraintestinal manifestations.
- Response to Treatment: In ITB, patients may show significant improvement with anti-tubercular therapy, whereas Crohn's Disease requires immunomodulators and biologics that target the dysregulated immune process.
Endoscopic and Biopsy Findings
Endoscopy with biopsy is often performed when the clinical and radiological picture is ambiguous:
- In ITB, colonoscopy might reveal transverse ulcers, circumferential involvement of the ileocecal region, and often caseating granulomas on histopathology. Acid-fast bacilli (AFB) studies, culture, or PCR may further support the diagnosis.
- In Crohn's Disease, colonoscopy could show longitudinal ulcers, aphthous lesions, and skip areas with intervening normal mucosa. Biopsies typically reveal non-caseating granulomas and features of chronic transmural inflammation.
Laboratory and Microbiological Investigations
In addition to imaging and endoscopic studies, laboratory work-up plays a critical role:
- Interferon-Gamma Release Assays (IGRA): Positive results would support a diagnosis of ITB, particularly when combined with clinical suspicion.
- Acid-Fast Bacillus (AFB) Staining and Culture: A definitive diagnosis of ITB can be made by isolating Mycobacterium tuberculosis from intestinal tissue.
- Inflammatory Markers: Both conditions may display elevated inflammatory markers, but a markedly high C-reactive protein (CRP) or erythrocyte sedimentation rate (ESR) may be more suggestive of an active inflammatory state as seen in Crohn's Disease.
Integrating CT Findings with Clinical Diagnosis
Weighing the Evidence
The CT scan findings present a nuanced picture that could be attributed to either ITB or Crohn's Disease. The homogeneously enhancing smooth mural thickening confined to the ileocecal region, along with minimal perilesional fat stranding and discrete lymph nodes, tends to favor an infectious process like ITB. However, similar features can occasionally be seen in early or mild Crohn's Disease, especially if the inflammatory process has not yet evolved into more characteristic chronic changes.
Arguments Favoring ITB
Several CT scan features in this study provide support for a diagnosis of ITB:
- The smooth and homogeneous nature of the mural thickening, coupled with its restricted anatomical involvement involving the terminal ileum, ileocecal junction, and proximal cecum, is typical for ITB.
- The minimal perilesional fat stranding observed aligns with a less aggressive inflammatory reaction as might be noted in ITB.
- The presence of discrete enhancing lymph nodes in the mesentery also supports ITB, especially if there were any hint of necrosis – although necrosis is not explicitly noted in this study, the overall enhancement pattern is more typical of an infectious lymphadenopathy.
Arguments Suggesting Crohn's Disease
Despite the CT characteristics leaning towards ITB, certain features may be aligned with early Crohn's Disease:
- In some cases of Crohn's Disease, the involvement may initially be confined to the ileocecal region with homogeneous thickening, particularly if complications such as skip lesions, transmural inflammation, or the comb sign have not yet developed.
- The diagnostic challenge is compounded in patients who do not display other characteristic clinical findings of either condition. In such scenarios, additional diagnostic tools are crucial for reaching a definitive handling strategy.
Role of Additional Diagnostic Evaluation
CT imaging, while incredibly valuable for providing an anatomical overview and clues to the underlying pathology, often requires supplementation with other diagnostic modalities to make a definitive diagnosis.
Endoscopic Evaluation and Biopsy
The next step in differentiating between ITB and Crohn's Disease involves endoscopic assessment of the gastrointestinal tract:
- Findings: Identification of ulcer patterns on colonoscopy – transverse and circumferential ulcers are more suggestive of ITB, whereas longitudinal, aphthous, and skip lesions point more towards Crohn's Disease.
- Biopsy Analysis: Histopathological examination can provide critical information. Caseating granulomas and positive AFB stains lean heavily towards ITB. In CD, non-caseating granulomas and chronic inflammatory changes without evidence of caseation are more common.
Laboratory Investigations
Complementary laboratory tests can add significant diagnostic value:
- Testing such as IGRA assays, cultures, and AFB staining are crucial for establishing ITB. A positive result for Mycobacterium tuberculosis would favor ITB.
- Inflammatory markers like CRP and ESR help gauge the activity of the inflammation, and while both conditions may show elevated levels, markedly high or fluctuating values in conjunction with clinical symptoms may be more indicative of Crohn's Disease.
Therapeutic and Prognostic Considerations
Treatment Response as a Diagnostic Aid
A pragmatic approach that many clinicians follow involves observing the patient’s response to empirical therapy:
Monitoring Treatment Response
Given the overlapping radiologic features, one practical strategy is to initiate specific treatment based on the most likely diagnosis and then monitor the patient’s clinical and radiological response:
- If ITB is suspected on the basis of supporting clinical and laboratory data, a trial of anti-tubercular therapy may be instituted. A significant clinical improvement and resolution of imaging findings over time can reinforce the ITB diagnosis.
- Conversely, if there is poor response to anti-tubercular therapy and signs of progressive inflammation or complications, this might prompt reconsideration of the diagnosis towards Crohn's Disease, leading to alternative treatment regimes including immunosuppressants or biologics.
Long-term Prognosis and Follow-up
Regardless of the definitive diagnosis, both ITB and Crohn's Disease require careful long-term follow up due to their potential for recurrence and complications:
- For ITB, monitoring ensures that the infection is fully treated and complications such as stricture formation are identified early.
- For Crohn's Disease, regular follow-up with imaging, endoscopy, and clinical assessment is critical to manage the chronicity of the condition and adjust therapy as needed, especially in patients prone to fistula, abscess, or stricturing complications.
Integration of Data and Final Assessment
Synthesizing the Clinical, Radiological, and Laboratory Findings
In summary, while the described CT scan findings – homogeneously enhancing smooth mural thickening involving the terminal ileum, ileocecal junction, and proximal cecum, minimal perilesional fat stranding, and discrete lymph nodes – present a challenging scenario where features of both ITB and Crohn's Disease overlap, the overall imaging pattern can slightly favor a diagnosis of ITB. Specifically, the homogeneity of the mural thickening and the nature of the lymphadenopathy are aspects that are more in line with ITB.
However, it is crucial to emphasize that the final diagnosis cannot be solely established on radiological grounds. Clinical details such as patient demographics, geographical background, systemic symptoms (e.g., fever, weight loss), history of tuberculosis exposure, and laboratory test results, when taken together with imaging findings, highly influence diagnostic accuracy.
The ambiguity further reaffirms the need for additional diagnostic procedures such as endoscopy with biopsy, targeted laboratory tests including AFB staining or culture and IGRA, and potentially a therapeutic trial to observe the response. Each of these steps contributes important pieces of evidence that help formulate a holistic view of the patient’s condition.
Given that Crohn's Disease typically may present with additional features such as segmental involvement, skip lesions, and more pronounced inflammatory fat changes during chronic phases, the absence of these in the present CT may lean the balance towards ITB. Nonetheless, only further clinical correlation – including histopathological confirmation – will provide definitive differentiation.
Conclusion and Final Thoughts
To definitively answer the question, "What can this CT scan be – ITB or Crohn's Disease?", the current CT scan findings with their presentation of smooth homogeneous mural thickening, minimal perilesional fat stranding, and discrete homogeneous lymph nodes seem to align more closely with intestinal tuberculosis (ITB). However, due to significant radiological overlap with early or mild forms of Crohn's Disease, further diagnostic evaluation is indispensable.
In clinical practice, the approach would typically include a detailed patient history, laboratory work-up including interferon-gamma release assays and acid-fast bacillus studies, along with endoscopic examination and biopsies to look for features such as caseating granulomas (favoring ITB) or non-caseating granulomas (favoring Crohn's Disease). In some cases, a trial of anti-tubercular therapy may also be used as a diagnostic tool, with an observed positive clinical response reinforcing the diagnosis of ITB.
Ultimately, while the CT findings raise a strong suspicion of ITB in this scenario, definitive diagnosis requires a holistic approach integrating imaging, clinical findings, and appropriate laboratory tests. Such an integrated diagnostic process is essential for initiating the correct treatment strategy and achieving improved patient outcomes.
References
-
PMC Article 1 - National Center for Biotechnology Information
-
PMC Article 2 - National Center for Biotechnology Information
- OUP Journal Article - ECCO Journal of Crohn's and Colitis
-
ScienceDirect Article - Gastroenterological Imaging
Recommended Further Reading
Last updated February 23, 2025