
Unlocking Precision Care: Mastering Hemodynamic Monitoring for Optimal Patient Outcomes
Navigate the complexities of hemodynamic assessment with expert insights for enhanced therapeutic decision-making.
Hemodynamic monitoring is a cornerstone of modern critical care and perioperative medicine, providing invaluable real-time insights into a patient's cardiovascular status. Effective utilization of these sophisticated tools allows clinicians to assess circulatory function, guide therapeutic interventions, and ultimately improve patient outcomes. This guide delves into the best practices for using hemodynamic monitors, from selecting the appropriate device to interpreting complex data and integrating it into a holistic treatment plan.
Highlights
- Tailor Monitor Selection: Choose the appropriate hemodynamic monitor by meticulously balancing the need for accuracy, the degree of invasiveness, and the specific clinical context and acuity of your patient.
- Integrate Data Holistically: Combine real-time hemodynamic parameters with a comprehensive clinical examination, laboratory assessments, and other diagnostic findings to form a complete and actionable understanding of the patient's condition.
- Leverage Dynamic Parameters: Utilize functional hemodynamic indicators such as Stroke Volume Variation (SVV) and Pulse Pressure Variation (PPV) to more accurately predict fluid responsiveness and guide fluid therapy, thereby optimizing cardiac performance and avoiding potential overload.
Navigating the Landscape: Choosing Your Hemodynamic Monitor
Selecting the right hemodynamic monitor is a critical first step. The choice depends on the patient's condition, the specific information needed, and the balance between the desired accuracy and acceptable invasiveness.
The Spectrum of Monitoring Technologies
Hemodynamic monitoring technologies range from completely non-invasive to highly invasive, each with its own set of applications, benefits, and limitations.
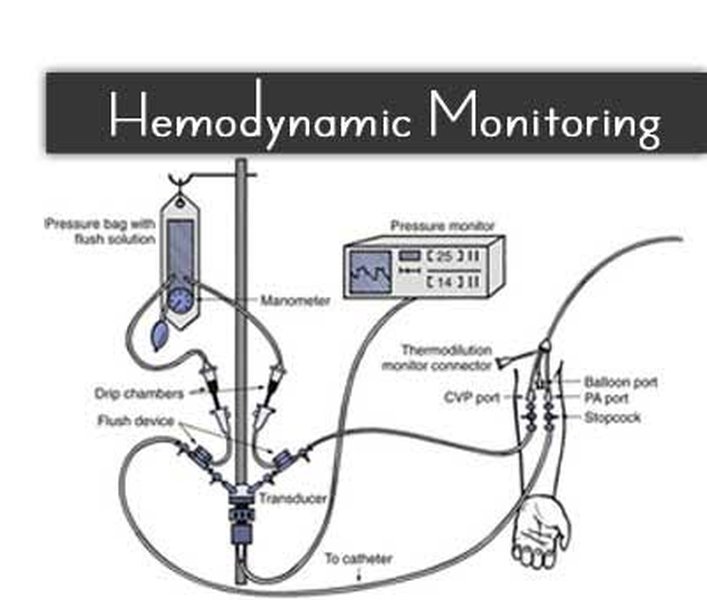
An array of hemodynamic monitoring equipment used in intensive care.
Non-Invasive Hemodynamic Monitoring
These methods provide physiological data without breaching the skin, minimizing patient risk and discomfort. They are often used for initial assessment or for patients who are relatively stable but require ongoing surveillance.
- Blood Pressure Cuffs (Automated): Provide intermittent systemic blood pressure readings. Advanced cuffs can offer more frequent measurements.
- Pulse Oximetry: Measures peripheral oxygen saturation (SpO2), offering insights into oxygenation status. Some advanced systems analyze the pulse oximeter waveform for additional hemodynamic data.
- Non-Invasive Cardiac Output (NICO) Devices: Employ techniques like bioreactance, bioimpedance, or pulse wave transit time to estimate cardiac output and other flow parameters without invasive lines.
- Echocardiography (Transthoracic - TTE): Uses ultrasound to visualize heart structures and blood flow, providing qualitative and quantitative assessment of cardiac function, valvular integrity, and volume status.
Minimally Invasive Hemodynamic Monitoring
These techniques typically involve an arterial line or specialized sensors, providing continuous and more detailed data than non-invasive methods, with less risk than fully invasive procedures.
- Arterial Pressure Waveform Analysis (Pulse Contour Analysis): Systems like FloTrac/Vigileo analyze the arterial pressure waveform, often obtained from a standard arterial line, to continuously estimate stroke volume (SV), cardiac output (CO), cardiac index (CI), and stroke volume variation (SVV). These require a good quality arterial signal.
- Esophageal Doppler Monitoring: A probe inserted into the esophagus measures blood flow velocity in the descending aorta to estimate cardiac output. It's particularly useful perioperatively for guiding fluid therapy.
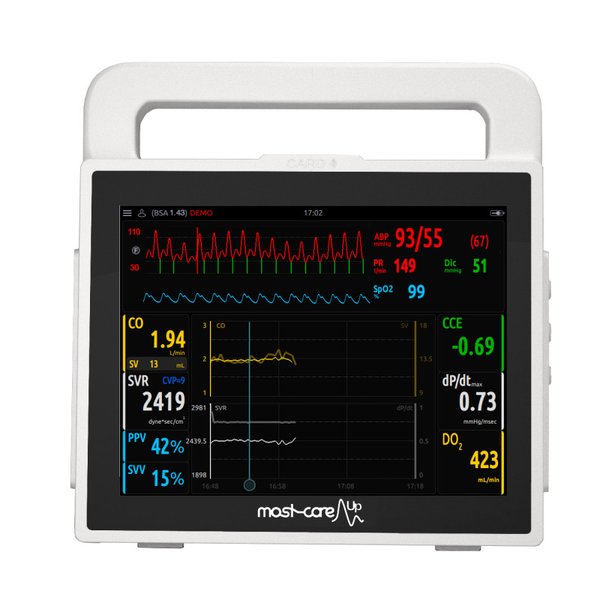
The MostCare Up monitor, an example of advanced hemodynamic monitoring technology using arterial pressure waveform analysis.
Invasive Hemodynamic Monitoring
Reserved for critically ill or high-risk surgical patients, these methods involve inserting catheters into major blood vessels or the heart for direct and precise measurements.
- Intra-Arterial Catheters (Art-lines): Provide continuous, beat-to-beat blood pressure monitoring and allow for frequent arterial blood gas sampling. Essential for patients on vasoactive infusions or with labile blood pressure.
- Central Venous Catheters (CVC): Measure central venous pressure (CVP), an indicator of right atrial pressure and right ventricular preload. Also provide access for fluid/drug administration and central venous oxygen saturation (ScvO2) measurement.
- Pulmonary Artery Catheter (PAC / Swan-Ganz Catheter): Considered a gold standard for complex cases, the PAC measures pulmonary artery pressures (PAP), pulmonary artery occlusion pressure (PAOP/PCWP - an estimate of left atrial pressure), cardiac output (via thermodilution), and mixed venous oxygen saturation (SvO2). It aids in differentiating shock states and guiding complex therapies.
Critical Factors in Monitor Selection
- Precision vs. Invasiveness: The ideal monitor offers maximum accuracy with minimal necessary invasiveness, tailored to the patient's risk profile.
- Patient Acuity and Clinical Question: Severely unstable patients or those with complex cardiopulmonary interactions often benefit from more comprehensive, invasive monitoring.
- Available Resources and Expertise: The choice may be influenced by equipment availability, staff familiarity, and institutional protocols.
- Comprehensive Parameters: The device should measure key variables related to preload, afterload, contractility, and oxygen transport to provide a complete cardiovascular assessment.
- Dynamic vs. Static Data: Preference is increasingly given to monitors that provide dynamic parameters predictive of fluid responsiveness.
The following chart offers a comparative overview of different hemodynamic monitoring modalities based on several key criteria. Higher scores on this radar chart generally indicate a more favorable characteristic (e.g., higher "Minimal Invasiveness" score means it is less invasive). This visualization can aid in understanding the trade-offs when selecting a monitor.
Mastering the Data: Key Hemodynamic Parameters & Interpretation
Understanding the array of parameters provided by hemodynamic monitors is crucial for effective clinical decision-making. These values, when interpreted in context, paint a detailed picture of the patient's cardiovascular performance.
This video provides a foundational understanding of the principles of hemodynamics, essential for interpreting monitor data.
Essential Parameters at a Glance
Blood Pressure (BP)
Mean Arterial Pressure (MAP) is a key perfusion pressure. Continuous invasive arterial BP monitoring is more accurate than NIBP in unstable patients, especially those on vasopressors or with severe vasoconstriction/dilation.
Cardiac Output (CO) and Cardiac Index (CI)
CO is the volume of blood pumped by the heart per minute (L/min). CI normalizes CO to body surface area (L/min/m²). These are vital indicators of overall cardiac function and systemic blood flow.
Preload Indicators (CVP, PAWP/PAOP)
Central Venous Pressure (CVP) reflects right ventricular filling pressure. Pulmonary Artery Wedge Pressure (PAWP) or Pulmonary Artery Occlusion Pressure (PAOP) estimates left ventricular filling pressure. While traditionally used to guide fluid therapy, their interpretation can be complex and they are increasingly supplemented or replaced by dynamic parameters.
Oxygen Delivery and Consumption (SvO2, ScvO2)
Mixed venous oxygen saturation (SvO2, from PAC) and central venous oxygen saturation (ScvO2, from CVC) indicate the balance between systemic oxygen delivery (DO2) and oxygen consumption (VO2). Low values can signal inadequate DO2 or increased VO2.
Dynamic Parameters for Fluid Responsiveness
These parameters predict whether a patient's cardiac output will increase with a fluid bolus. They are generally more reliable than static filling pressures in mechanically ventilated patients.
- Stroke Volume Variation (SVV): The variation in stroke volume over the respiratory cycle.
- Pulse Pressure Variation (PPV): The variation in pulse pressure over the respiratory cycle.
- Passive Leg Raise (PLR): A reversible maneuver that mimics a fluid challenge by increasing venous return.
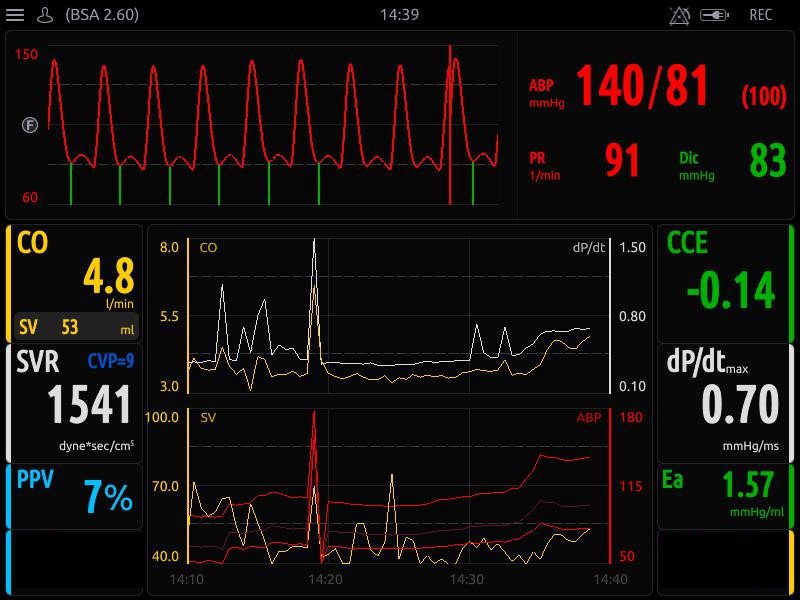
A modern hemodynamic monitor interface displaying various cardiovascular parameters, including dynamic indices.
Beyond the Numbers: The Art of Interpretation
Hemodynamic data should never be interpreted in isolation. Effective use involves:
- Contextualization: Consider the patient's underlying physiology, comorbidities, current therapies, and overall clinical picture.
- Trend Analysis: Single values are less informative than trends over time, which indicate response to therapy or deterioration.
- Understanding Limitations: Be aware of potential artifacts, measurement errors, and the specific limitations of each parameter and device. For example, dynamic parameters have reduced reliability in patients with spontaneous breathing, arrhythmias, or right heart failure.
- Dynamic vs. Static Measures: Prioritize dynamic assessments of fluid responsiveness over static filling pressures when making decisions about fluid administration.
From Data to Action: Clinical Applications and Therapeutic Guidance
The ultimate goal of hemodynamic monitoring is to guide therapies that optimize tissue perfusion and oxygen delivery, thereby improving patient outcomes in various critical conditions.
Guiding Life-Saving Interventions
Fluid Management
Hemodynamic monitors, particularly those providing dynamic parameters (SVV, PPV) or enabling fluid challenge assessments (e.g., passive leg raise with CO monitoring), help determine if a patient is fluid-responsive. This guides judicious fluid administration, aiming to optimize cardiac output while avoiding the deleterious effects of fluid overload.
Vasoactive Drug Administration
Continuous monitoring of MAP, CO, and systemic vascular resistance (SVR, often calculated) allows for precise titration of vasopressors (to increase MAP) and inotropes (to improve contractility and CO) based on the patient's specific hemodynamic profile and therapeutic targets.
Mechanical Circulatory Support Decisions
In cases of severe cardiogenic shock refractory to medical therapy, detailed hemodynamic data from invasive monitors (e.g., PAC) can help identify the need for and guide the management of mechanical circulatory support devices like intra-aortic balloon pumps (IABP) or ventricular assist devices (VADs).
Tailoring Care in Specific Clinical Scenarios
- Shock States: Hemodynamic monitoring is crucial for diagnosing the type of shock (hypovolemic, cardiogenic, obstructive, distributive/septic) by assessing parameters like CO, CVP, PAWP, and SVR. This allows for targeted therapy.
- Sepsis and Septic Shock: Guiding early fluid resuscitation, vasopressor use, and assessing tissue perfusion (e.g., via ScvO2 or lactate clearance) are key applications.
- Heart Failure: Monitoring helps assess volume status, cardiac function, and response to diuretics, vasodilators, and inotropes. Implantable hemodynamic monitors are emerging for chronic management to detect early decompensation.
- Perioperative Management: Particularly in high-risk surgery, goal-directed therapy based on parameters like CO, SVV, and DO2 can help reduce complications and length of stay.
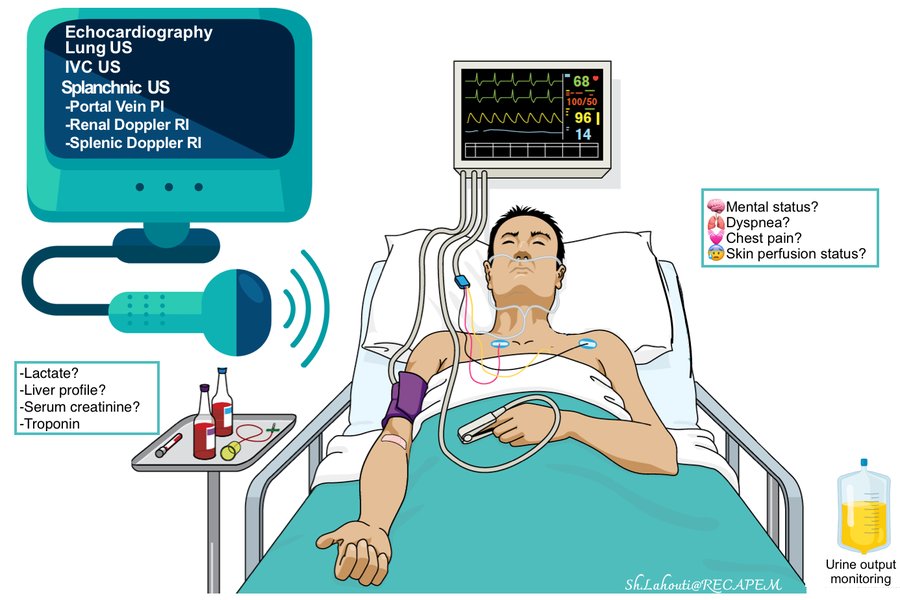
Echocardiography plays an increasingly important role in contemporary hemodynamic assessment, often complementing other monitoring modalities.
Optimizing Outcomes: Advanced Strategies and Best Practices
Maximizing the benefits of hemodynamic monitoring requires more than just choosing a device and reading numbers. It involves a systematic approach, continuous learning, and integration into broader care strategies.
The following mindmap illustrates the comprehensive decision-making process involved in utilizing hemodynamic monitoring effectively, from initial patient assessment through to therapeutic interventions and ongoing re-evaluation.
The Power of Protocol-Driven Care
Implementing goal-directed therapy (GDT) protocols that link specific hemodynamic targets to interventions has been shown to improve outcomes in certain patient populations, such as high-risk surgical patients or those with septic shock. These protocols help standardize care and ensure timely adjustments.
Ensuring Data Integrity: Signal Quality and Calibration
The adage "garbage in, garbage out" holds true. For monitors relying on arterial pressure waveforms, meticulous attention to the arterial line setup is crucial to prevent damping or resonance, which can distort the waveform and lead to inaccurate derived parameters. Regular calibration and zeroing of transducers are essential for all invasive pressure monitoring.
The Human Element: Training and Multidisciplinary Teams
Proficiency in operating hemodynamic monitoring devices and interpreting their data requires ongoing education and training for all healthcare professionals involved. A multidisciplinary team approach, involving physicians, nurses, and respiratory therapists, facilitates comprehensive assessment and coordinated care.
The Future is Now: Emerging Technologies
- Implantable Hemodynamic Monitors: Devices like the CardioMEMS HF System allow for chronic remote monitoring of pulmonary artery pressures in heart failure patients, enabling proactive management and potentially reducing hospitalizations.
- Artificial Intelligence (AI) and Decision Support: Advanced software platforms are being developed to integrate multiple hemodynamic parameters, predict instability, and provide clinical decision support, helping clinicians process complex data more efficiently.
Comparative Overview of Hemodynamic Monitoring Modalities
The table below provides a summary comparison of different hemodynamic monitoring techniques, highlighting their key characteristics, parameters measured, and common clinical applications.
| Modality | Description | Key Parameters Measured | Invasiveness | Primary Use Cases | Advantages | Limitations |
|---|---|---|---|---|---|---|
| Non-Invasive Blood Pressure (NIBP) Cuff | Automated oscillometric cuff | Systolic, Diastolic, Mean Arterial Pressure (MAP), Heart Rate | Non-invasive | Routine monitoring, stable patients | Easy to use, low risk | Intermittent, less accurate in shock/arrhythmias |
| Pulse Oximetry | Measures peripheral oxygen saturation | SpO2, Pulse Rate | Non-invasive | Routine oxygenation monitoring | Easy to use, continuous | Affected by poor perfusion, motion artifact, dyshemoglobinemias |
| Arterial Line (Intra-arterial Catheter) | Catheter in an artery | Continuous BP, MAP; allows for arterial blood gas sampling; input for pulse contour analysis | Invasive | Unstable BP, frequent ABGs, vasoactive drugs, pulse contour CO monitoring | Continuous, accurate BP, access for blood sampling | Risks (infection, thrombosis, hematoma), requires skill |
| Central Venous Catheter (CVC) | Catheter in a large central vein | Central Venous Pressure (CVP), Central Venous Oxygen Saturation (ScvO2) | Invasive | Volume status assessment (with caution), ScvO2 monitoring, drug/fluid administration | Central access, ScvO2 insight | Risks (infection, pneumothorax), CVP poor predictor of fluid responsiveness alone |
| Pulmonary Artery Catheter (PAC) | Flow-directed catheter into pulmonary artery | PAP, PAOP/PCWP, CO (thermodilution), SvO2, CVP, SVR/PVR (calculated) | Highly invasive | Complex shock, severe heart failure, ARDS, pulmonary hypertension, major cardiac surgery | Comprehensive data, direct intracardiac pressures | High risk (arrhythmias, PA rupture), requires expertise, controversial impact on routine outcomes |
| Pulse Contour Analysis (Minimally Invasive CO) | Analyzes arterial waveform from arterial line | Continuous CO, CI, SV, SVV, PPV, SVR (some systems) | Minimally invasive (requires arterial line) | Perioperative goal-directed therapy, sepsis, guiding fluid/vasoactive therapy | Continuous CO, dynamic parameters | Requires good arterial signal, less accurate in severe arrhythmias, vasoplegia, aortic regurgitation |
| Esophageal Doppler | Probe in esophagus measures aortic blood flow velocity | CO, SV, Flow Time Corrected (FTc) | Minimally invasive | Perioperative fluid optimization, ICU patients | Less invasive CO, responsive to changes | Probe placement critical, operator dependent, affected by patient position |
| Echocardiography (TTE/TEE) | Ultrasound imaging of the heart | Cardiac structure/function, valvular disease, pericardial effusion, EF, CO (Doppler-derived), volume status assessment | Non-invasive (TTE) / Minimally invasive (TEE) | Diagnosis of shock etiology, assessing cardiac function, guiding fluid resuscitation | Rich anatomical and functional data, non-invasive option | Operator dependent, may be intermittent, TEE is semi-invasive |
Frequently Asked Questions (FAQ)
Conclusion
The effective use of hemodynamic monitors is a multifaceted skill that blends technological understanding with astute clinical judgment. By carefully selecting the appropriate monitoring modality, meticulously ensuring data quality, interpreting parameters within the broader clinical context, and integrating these insights into protocol-driven, individualized therapeutic strategies, clinicians can significantly enhance their ability to manage critically ill patients. As technology continues to advance, a commitment to continuous learning and a holistic approach to patient assessment will remain paramount in leveraging hemodynamic monitoring to its fullest potential for improving patient outcomes.
Recommended
- What are the detailed pros and cons when comparing invasive versus non-invasive hemodynamic monitoring techniques?
- How can I accurately interpret stroke volume variation (SVV) and pulse pressure variation (PPV) in guiding fluid therapy for mechanically ventilated patients?
- What is the specific role and utility of the Pulmonary Artery Catheter (PAC) in the contemporary management of cardiogenic shock?
- What are the latest advancements and clinical impact of implantable hemodynamic monitors for patients with chronic heart failure?
