
Anatomy and Physiology of the Neonatal Gastrointestinal System
A Comprehensive Overview for Understanding Newborn GI Structure and Function
Highlights
- Rapid Postnatal Adaptation: The neonatal GI tract undergoes dynamic structural and functional changes shortly after birth.
- Maturity Challenges: The immaturity of digestive enzymes, motility, and barrier function impacts feeding and nutrient absorption.
- Microbiome and Immunity Integration: Early microbial colonization plays a crucial role in immune development and GI maturation.
Introduction
The neonatal gastrointestinal (GI) system represents a remarkable model of rapid developmental transformation. This transition brings the fetus from a placental nutrient supply to self-sufficient enteral nutrition shortly after birth. The intricate interplay of anatomical structure, physiological function, and evolving immune mechanisms defines neonatal GI health. Here, we explore the multiple facets of the neonatal GI system—including its developmental anatomy, functional physiology, challenges for preterm infants, and the pivotal role of the gut microbiome—in order to understand its impact on feeding, digestion, and overall immune defense.
Developmental Anatomy of the Neonatal GI System
Embryological Origins and Postnatal Adaptation
The neonatal GI tract originates from the primitive digestive tube that develops from the yolk sac during embryogenesis. Key phases in its development occur during the second and third trimesters of pregnancy, where the intestine undergoes considerable lengthening and morphological changes. At birth, the anatomical components include the oropharynx, esophagus, stomach, and the extensive small and large intestines.
Segmental Organization
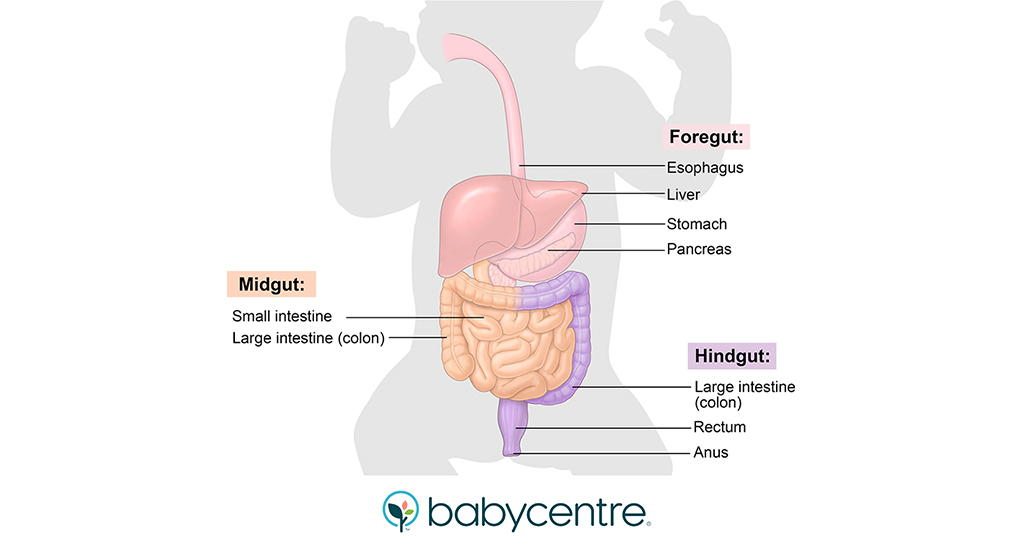
The GI tract is organized into three main segments:
- Foregut: Gives rise to the esophagus, stomach, liver, pancreas, and proximal duodenum.
- Midgut: Develops into the distal duodenum, jejunum, ileum, cecum, appendix, and the proximal portion of the colon.
- Hindgut: Forms the remainder of the colon and the upper segment of the anal canal.
Though the overall length of the neonatal GI tract is relatively short compared to adults, rapid postnatal growth is an essential aspect of its maturation. For instance, while the small intestine measures approximately 275 cm at term, it increases substantially in length during early childhood.
Physiological Functions and Processes
Digestive Mechanisms and Nutrient Absorption
The primary functions of the neonatal GI system include the digestion of nutrients and their absorption for growth and metabolism. The neonatal gut is specially adapted to process colostrum and breast milk, which are rich in easily digestible nutrients like lactose, proteins, and fats. However, due to the immaturity of the digestive enzymes and the structure of the intestinal villi, the efficiency of complex carbohydrate or protein digestion is often limited until later developmental phases.
Digestive Enzymes and Brush Border Maturation
Newborns are equipped with key enzymes necessary for the digestion of breast milk. Lactase, in particular, is present in high concentrations to break down lactose efficiently. In contrast, the enzymes required to digest more complex substrates are expressed at lower levels, reflecting the adaptation to a milk-based diet. Additionally, the intestinal lining, with its microvilli and villi structures, provides an extensive surface area for nutrient absorption. These structures, although present at birth, continue to mature postnatally.
Gastric Motility and Emptying
Gastric motility in neonates is generally slower than in adults due to an underdeveloped muscular system. This slower motility necessitates more frequent, smaller feedings to avoid overwhelming the immature stomach and to ensure adequate nutrient absorption. The process of gastric emptying gradually improves with increasing gestational age, yet remains an important consideration, particularly in preterm infants who face substantial challenges in this regard.
Challenges in Preterm Neonates
Implications of Immaturity
Preterm neonates exhibit several distinct challenges related to their underdeveloped GI systems. These infants often experience:
- Delayed Gastric Emptying: Slower emptying times can lead to issues such as feeding intolerance and increased risk of reflux.
- Limited Digestive Enzyme Activity: Inadequate levels of enzymes reduce the efficiency of nutrient digestion and absorption.
- Underdeveloped Intestinal Motility: A less coordinated muscular activity in the intestinal wall can impede the smooth transit of food, contributing to feeding difficulties.
- Compromised Barrier Function: A developing gut barrier increases vulnerability to infections and conditions such as necrotizing enterocolitis (NEC).
Nutritional management in these infants requires special consideration, including the administration of small, frequent feeds and the careful monitoring of nutrient uptake. Such strategies help cater to the limited absorptive capacity of the preterm GI tract.
Clinical Management and Implications
Given these developmental challenges, healthcare professionals often adopt targeted nutritional strategies for preterm infants. These strategies may involve:
- Parenteral Nutrition: Used when enteral feeding is insufficient or contraindicated, ensuring that the infant receives essential nutrients while the GI system continues to mature.
- Gentle Feeding Protocols: Employing slower, gradual increases in feed volumes to allow the GI tract to adapt and develop its full range of digestive function.
- Probiotic Administration: Enhancing the gut microbiome to support immune function and improve overall GI health.
Neonatal Gastrointestinal Motility and Coordination
Mechanisms Behind Movements
Gastrointestinal motility in neonates is controlled by a network of smooth muscle contractions, neural inputs, and hormonal signals. Various hormones, including ghrelin, secretin, and pancreatic peptides, aid in regulating digestive processes. In the early neonatal period, this coordination is still maturing, contributing to the varied rates of gastric emptying and intestinal transit.
Intestinal Peristalsis
Peristalsis—the wave-like contractions that move food along the GI tract—is less rhythmic and robust in newborns. While full-term neonates may exhibit a pattern closer to the norm, preterm infants often exhibit irregular contractions that can hinder effective digestion and transit of food.
Interplay Between Neural and Hormonal Control
The neonatal GI system is gradually integrating the autonomic nervous system inputs with hormonal signals over the first few weeks of life. This coordinated system is pivotal in tuning functions like secretion of digestive juices, modulation of intestinal motility, and the absorbent functions of the gut.
The Role of the Gut Microbiome and Immunity
Establishment of a Protective Microbial Ecosystem
One of the most transformative events in neonatal life is the establishment of the gut microbiome. Initially, the neonatal gut is sterile, but colonization begins immediately after birth. The mode of delivery (vaginal versus cesarean) and the type of feeding (breast milk versus formula) significantly influence the composition of the microbial population.
Microbiome Development
The colonization of the neonatal gut with bacteria, viruses, and fungi is critical not only for digestion but also for immune system programming. Beneficial bacteria help protect against pathogens by forming a competitive barrier and stimulating the development of the gut-associated lymphoid tissue (GALT). As the microbiome matures, it plays a central role in modulating local and systemic immune responses.
Immune-Barrier Functions
The neonatal intestinal barrier is in a phase of active development. Initially more permeable compared to an adult’s barrier, it gradually improves through cellular maturation and microbial interactions. This evolving barrier function is vital in preventing the translocation of pathogens while enabling the appropriate absorption of nutrients and immunoglobulins.
Integrative Comparison: Term vs. Preterm Neonates
Detailed Comparison Table
The following table summarizes key differences in GI anatomy and physiology between term and preterm neonates:
| Characteristic | Term Neonates | Preterm Neonates |
|---|---|---|
| GI Tract Maturity | More developed anatomical structures and enzyme levels for digesting milk | Limited enzyme activity; underdeveloped structural features |
| Gastric Emptying | Relatively efficient with frequent small feedings | Slower gastric emptying, resulting in feeding intolerance |
| Intestinal Motility | Better coordinated peristalsis aiding nutrient transit | Inefficient and irregular motility patterns |
| Immune Barrier | Improving barrier functions with gradual microbial colonization | Increased permeability and susceptibility to infections |
| Microbiome Establishment | Robust microbiome development influenced by breastfeeding | Delayed and abnormal microbial colonization, often necessitating probiotics |
Hormonal Control and Regulatory Mechanisms
Endocrine Influences on GI Function
Hormonal signals play a critical role in modulating the GI function of neonates. Hormones such as ghrelin, secretin, and various pancreatic hormones help regulate the secretion of digestive enzymes and the motility of the gut. They also influence appetite, determining the frequency and preferences of neonatal feeding.
Ghrelin and Secretin Interaction
Ghrelin, known for its role in stimulating hunger, interacts with the neonatal gut to modulate energy balance. Concurrently, secretin helps regulate the pancreatic secretion of bicarbonate and enzymes which are essential for buffering the acidic environment of the stomach and facilitating digestion.
Pancreatic Hormones
Pancreatic hormones are crucial for releasing digestive enzymes. The gradual increase in the activity and coordination of these enzymes further supports the evolving capacity of the GI tract to break down nutrients effectively.
Nutrition, Feeding Strategies, and Medication Absorption
Adapting to Enteral Feeding
The shift from in utero placental nutrition to enteral feeding presents a series of challenges and adaptations. The neonatal GI tract must quickly learn to process either colostrum, breast milk, or formula—each containing nutrients in different proportions. Their digestive systems are optimized for the high lactose and fat content of human milk. However, the immaturity of the intestines and digestive enzyme levels requires careful management of feeding volumes and timing, particularly in preterm neonates.
Feeding Strategies for Healthy Neonatal Development
Several feeding strategies have been developed to help mitigate the limitations of the immature GI tract:
- Frequent Small Volume Feeds: Favors the slow yet steady digestibility and gradual stimulation of peristalsis.
- Parenteral Nutrition: Employed for neonates unable to tolerate full enteral feeds or who have compromised gut barrier function.
- Supplementation with Probiotics: Aims to promote the early establishment of a beneficial gut microbiome, thereby supporting immune and digestive health.
Medication Absorption Considerations
Medication absorption in neonates is influenced by the developmental stage of the GI tract. Drugs administered orally must navigate an immature digestive landscape, affecting the rate and efficiency of absorption. Understanding these variations is essential when dosing medications for neonates, particularly in cases with altered gastric pH, variable enzyme activity, and delayed intestinal clearance.
Special Considerations and Pathological Conditions
Common Clinical Challenges
In addition to the typical developmental issues, neonates, especially those born preterm, may encounter specific pathological conditions. Key among these is necrotizing enterocolitis (NEC), a potentially life-threatening condition characterized by inflammation and necrosis of intestinal tissue. Additionally, disorders such as Hirschsprung’s disease—marked by a lack of ganglion cells in segments of the colon—may result in intestinal obstruction and require early interventions.
Necrotizing Enterocolitis (NEC)
NEC primarily affects the most vulnerable, preterm infants with compromised barrier integrity and abnormal intestinal motility. Preventative measures include controlled feeding protocols and the strategic use of probiotics to support a balanced gut microbiome.
Other Gastrointestinal Disorders
Gastroesophageal reflux, though common in both term and preterm neonates, may require more sensitive management in preterm infants. The clinical approach ranges from dietary modifications to pharmacological interventions aimed at reducing gastric acidity and improving sphincter tone.
Research and Future Directions
Ongoing Studies and Emerging Insights
The field of neonatal gastroenterology is continuously evolving with advancements in medical research. Current studies are focusing on including detailed analysis of the neonatal gut microbiome and its long-term effects on health, as well as the optimization of feeding protocols tailored to the individual needs of neonates. Further research into the hormonal regulation and enzymatic maturation of the GI tract is expected to improve clinical outcomes, particularly in vulnerable preterm populations.
Innovative Nutritional Approaches
Emerging nutritional strategies aim to provide precisely balanced nutrients that support not only the growth of neonates but also the maturation of the gut’s enzymatic and immune defenses. Custom-tailored nutritional supplements and bioactive compounds derived from human milk are being researched for their potential roles in enhancing gut barrier function and promoting healthy microbiome development.
Technological Advances in Neonatal Care
Advanced imaging technologies and novel biomarker analyses are on the forefront of assessing the functional maturity of the neonatal GI system. These advancements allow clinicians to better predict feeding outcomes and personalize interventions, ensuring that each neonate receives the most suitable form of nutritional support and medication dosing.
References
- Physiology of the Neonatal Gastrointestinal System - PubMed
- Disposition of Orally Administered Medications - Drug Metabolism & Disposition
-
Development of the Gastrointestinal Tract in Newborns - PMC
- Physiology of the Gastrointestinal Tract in Newborns - SpringerLink
- The Neonatal Gastrointestinal Tract - NeoReviews
Recommended Queries
Last updated March 9, 2025