
Beyond the Heart Attack: Understanding the Critical Aftermath
Exploring the crucial short-term and long-term complications that can follow a myocardial infarction.
A myocardial infarction (MI), commonly known as a heart attack, occurs when blood flow to a part of the heart muscle is blocked, causing damage or death to heart tissue. While immediate survival is the primary concern, the period following an MI is critical due to the potential for various complications, known as post-MI sequelae. These sequelae can range from immediate, life-threatening events to chronic conditions that develop over weeks, months, or even years, significantly impacting heart function, quality of life, and long-term prognosis.
Key Insights into Post-MI Sequelae
- Diverse Complications: Post-MI sequelae encompass a wide spectrum, including mechanical failures (like heart wall rupture), electrical disturbances (arrhythmias), pump dysfunction (heart failure), inflammatory responses (pericarditis), and long-term structural changes (remodeling).
- Timing Matters: Complications can arise acutely (within hours to days), subacutely (within days to weeks), or chronically (weeks to years later). Early reperfusion therapy (restoring blood flow quickly) significantly reduces the risk and severity of many sequelae.
- Prognostic Significance: The presence and type of post-MI sequelae are major determinants of long-term survival and quality of life. Detecting and managing these complications promptly is crucial for improving outcomes.
Acute Complications: The Immediate Aftermath (Hours to Weeks)
The period immediately following an MI is fraught with potential dangers as the damaged heart muscle is vulnerable and inflammatory processes are initiated. Early recognition and management of these acute sequelae are vital.
Mechanical Complications: Structural Failures
These are among the most feared complications, often resulting from the physical tearing or rupture of weakened heart tissue. While less common in the era of rapid reperfusion, they remain life-threatening emergencies.
Myocardial Rupture
Myocardial rupture typically occurs 3-7 days post-MI, when the necrotic (dead) tissue is weakest due to enzymatic degradation and inflammatory cell infiltration, but before significant scar tissue has formed. Types include:
- Left Ventricular Free Wall Rupture (FWR): A tear in the outer wall of the left ventricle. This can lead to hemopericardium (blood filling the sac around the heart) and cardiac tamponade (compression of the heart), often causing sudden death. Incidence is around 0.01–0.52% but carries extremely high mortality.
- Ventricular Septal Rupture (VSR): A hole develops in the wall (septum) separating the left and right ventricles. This creates a left-to-right shunt, causing oxygenated blood to mix with deoxygenated blood, leading to right ventricular volume overload, heart failure, and potentially cardiogenic shock. It presents with a new, loud holosystolic murmur and occurs in about 0.17–0.91% of MIs.
- Papillary Muscle Rupture (PMR): The papillary muscles anchor the mitral valve leaflets. If one ruptures (partially or completely), it causes acute severe mitral regurgitation (blood leaking backward into the left atrium). This sudden volume overload on the left atrium and lungs leads to pulmonary edema and shock. It presents with a holosystolic murmur radiating to the axilla and affects 0.05–0.26% of MI patients.
The risk of rupture is higher with large infarcts, delayed reperfusion, female sex, older age, and first-time MIs. Treatment typically requires emergency surgical repair.
Other Mechanical Issues
- Left Ventricular Pseudoaneurysm: This occurs when a free wall rupture is contained by adherent pericardium or scar tissue, forming a blood-filled sac outside the ventricle that communicates with the ventricular cavity through a narrow neck. Unlike a true aneurysm, its wall lacks myocardial tissue and is prone to rupture.
- Dynamic Left Ventricular Outflow Tract (LVOT) Obstruction: In some cases, especially with anterior MIs, the non-infarcted base of the heart may become hypercontractile, leading to obstruction of blood flow out of the left ventricle during systole, mimicking hypertrophic cardiomyopathy and worsening heart failure symptoms.
Arrhythmic Complications: Electrical Instability
Damage to the heart muscle and its electrical conduction system is common after MI, leading to various arrhythmias.
- Ventricular Arrhythmias: Ventricular tachycardia (VT) and ventricular fibrillation (VF) are life-threatening rhythms that can cause sudden cardiac death, particularly in the first 48 hours post-MI. They result from irritable ischemic tissue or re-entry circuits around the infarct scar.
- Supraventricular Arrhythmias: Atrial fibrillation (AF) is common, increasing the risk of stroke due to potential clot formation in the atria.
- Bradyarrhythmias and Heart Block: Damage to the sinoatrial (SA) node, atrioventricular (AV) node, or bundle branches can cause slow heart rates (bradycardia) or conduction blocks. Inferior MIs are often associated with transient AV block due to increased vagal tone or ischemia of the AV node (often supplied by the right coronary artery). Anterior MIs can cause more permanent damage to the bundle branches.
Pump Failure and Hemodynamic Instability
Significant loss of contractile muscle can impair the heart's ability to pump blood effectively.
- Acute Heart Failure: Symptoms like shortness of breath (dyspnea), fatigue, and fluid retention (edema) can develop rapidly if a large portion of the ventricle is damaged. This can be left-sided, right-sided, or bilateral.
- Cardiogenic Shock: This is the most severe form of pump failure, where the heart cannot pump enough blood to meet the body's needs, leading to low blood pressure, organ damage, and high mortality. It often occurs with large anterior MIs or significant right ventricular involvement.
- Right Ventricular (RV) Infarction: Occurring in about 16% of MIs, particularly with inferior MIs involving the right coronary artery, RV infarction can lead to right-sided heart failure (jugular venous distension, peripheral edema) and hypotension, complicating management.
Inflammatory Complications
The body's inflammatory response to tissue injury can affect the pericardium (the sac surrounding the heart).
- Early Pericarditis: Inflammation of the pericardium occurring within the first few days post-MI, affecting up to 40% of patients (especially with larger, transmural infarcts). It causes sharp, pleuritic chest pain (worse with breathing or lying down, relieved by sitting up) and a characteristic pericardial friction rub may be heard on auscultation.
- Pericardial Effusion: Fluid accumulation within the pericardial sac, seen in up to 66% of cases post-MI. Small effusions are common and benign, but large or rapidly accumulating effusions can lead to cardiac tamponade.
Ischemic Complications
Ongoing or recurrent ischemia can occur.
- Infarct Extension/Re-infarction: The area of infarction may enlarge, or a new infarction may occur in a different area, often presenting with recurrent chest pain, new ECG changes, and further elevation of cardiac biomarkers.
- Post-infarction Angina: Recurrent chest pain after MI, indicating residual ischemia in the infarct-related artery territory or significant disease in other coronary arteries.
Microvascular Obstruction (MO)
Even after successfully reopening the main infarct-related artery (e.g., via PCI), blood flow may not be fully restored at the capillary level within the infarct zone. This 'no-reflow' phenomenon, termed microvascular obstruction, is due to capillary damage, swelling, and plugging. MO is associated with larger infarcts, poorer ventricular function recovery, adverse remodeling, and worse long-term prognosis. It can be detected using techniques like cardiac MRI.
Chronic Complications: The Long-Term Legacy (Weeks to Years)
As the acute phase subsides, the heart undergoes healing and remodeling processes that can lead to long-term structural and functional changes.
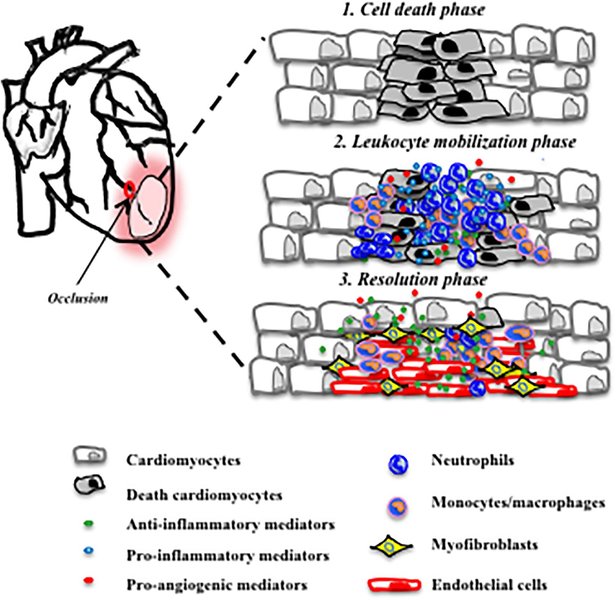
The complex process of inflammation, healing, and scar formation following myocardial infarction.
Ventricular Remodeling
This refers to changes in the size, shape, and thickness of the left ventricle after an MI. While some remodeling is adaptive, adverse remodeling involves progressive chamber dilation, thinning of the infarct scar, and hypertrophy (thickening) of the remaining viable muscle. This process is driven by mechanical stress, neurohormonal activation, and inflammatory factors. Adverse remodeling impairs contractile function, increases wall stress, and is a major driver for the development and progression of chronic heart failure.
Chronic Heart Failure
This is a common long-term sequela, resulting from the irreversible loss of contractile muscle and adverse remodeling. Patients experience progressive symptoms like dyspnea, fatigue, exercise intolerance, and fluid retention, requiring long-term medical management.
Left Ventricular Aneurysm
A true aneurysm is a late complication where a thinned, scarred section of the ventricular wall bulges outward during systole. Unlike a pseudoaneurysm, its wall consists of fibrous scar tissue and non-functional myocardium. While rupture is rare, true aneurysms can lead to heart failure, ventricular arrhythmias, and thrombus formation within the aneurysm sac.
Thromboembolic Complications
Blood can stagnate in areas of poor contraction, such as an akinetic (non-moving) segment or an aneurysm, leading to the formation of a left ventricular mural thrombus (clot attached to the heart wall). Pieces of this thrombus can break off and embolize, traveling through the bloodstream to block arteries elsewhere, most commonly causing stroke, but also potentially affecting limbs or organs.
Dressler Syndrome (Post-Myocardial Infarction Syndrome)
This is a delayed form of pericarditis, typically occurring weeks to months after an MI. It's believed to be an autoimmune reaction to cardiac antigens released from damaged heart muscle. Symptoms include fever, pleuritic chest pain, pericardial effusion, and sometimes pleural effusions (fluid around the lungs). It usually responds well to anti-inflammatory medications.
Chronic Arrhythmias
The scar tissue formed during healing can disrupt normal electrical conduction pathways, creating circuits that predispose patients to sustained ventricular tachycardia or fibrillation, increasing the long-term risk of sudden cardiac death.
Psychological Sequelae
Surviving a heart attack is a major life event that can have significant psychological impacts. Depression, anxiety disorders, and post-traumatic stress disorder (PTSD) are common in the months following an MI, affecting recovery, adherence to treatment, and overall quality of life.
Visualizing the Landscape of Post-MI Sequelae
Relative Risk and Impact Over Time
The following chart provides a conceptual overview of the relative risk or impact of different categories of post-MI sequelae during different phases after the event. Note that this represents general trends and individual patient experiences can vary significantly based on infarct size, location, treatment, and comorbidities. The scale reflects relative impact rather than absolute incidence.
As illustrated, mechanical complications and acute life-threatening arrhythmias pose the greatest immediate risk. Over time, the impact shifts towards complications related to structural changes like adverse remodeling, chronic heart failure, thromboembolism, and persistent arrhythmias.
Mapping the Connections: A Mindmap Overview
This mindmap provides a structured overview of the primary categories and specific examples of post-myocardial infarction sequelae, illustrating the diverse nature of these complications.
(Hours to Weeks)"] Mechanical["Mechanical"] FWR["Free Wall Rupture"] VSR["Ventricular Septal Rupture"] PMR["Papillary Muscle Rupture"] Pseudoaneurysm["Pseudoaneurysm"] LVOT_Obs["Dynamic LVOT Obstruction"] Arrhythmic["Arrhythmic"] VT_VF["Ventricular Tachycardia / Fibrillation"] AF["Atrial Fibrillation"] Blocks["Heart Blocks / Bradycardia"] Pump_Failure["Pump Failure"] Acute_HF["Acute Heart Failure"] Card_Shock["Cardiogenic Shock"] RV_Infarct["RV Infarction"] Inflammatory["Inflammatory"] Early_Peri["Early Pericarditis"] Per_Effusion["Pericardial Effusion"] Ischemic["Ischemic"] Infarct_Ext["Infarct Extension / Re-infarction"] Post_MI_Angina["Post-MI Angina"] Microvascular["Microvascular Obstruction (MO)"] Chronic_Complications["Chronic Complications
(Weeks to Years)"] Remodeling["Ventricular Remodeling"] Dilation["LV Dilation"] Aneurysm["True LV Aneurysm"] Chronic_HF["Chronic Heart Failure"] Thromboembolic["Thromboembolic"] LV_Thrombus["LV Mural Thrombus"] Embolism["Systemic Embolism (Stroke)"] Chronic_Arrhythmia["Chronic Arrhythmias"] Dressler["Dressler Syndrome"] Psychological["Psychological"] Depression["Depression"] Anxiety["Anxiety"] PTSD["PTSD"]
Summary of Key Post-MI Sequelae
This table summarizes the major categories of complications following a myocardial infarction, providing examples, typical timing, and clinical significance.
| Category | Specific Examples | Typical Timeline | Clinical Significance & Key Features |
|---|---|---|---|
| Mechanical | LV Free Wall Rupture, Ventricular Septal Rupture (VSR), Papillary Muscle Rupture (PMR) | Acute (esp. days 3-7 for rupture) | Life-threatening emergencies often requiring urgent surgery; associated with tamponade, shock, acute heart failure, new murmurs. Incidence reduced by early reperfusion. |
| Arrhythmic | Ventricular Tachycardia/Fibrillation (VT/VF), Atrial Fibrillation (AF), Heart Block, Bradycardia | Acute (esp. first 48h for VT/VF), can become Chronic | Risk of sudden cardiac death (VT/VF), stroke (AF), hemodynamic compromise. Scar tissue can be a substrate for chronic arrhythmias. |
| Pump Failure | Acute Heart Failure, Cardiogenic Shock, Right Ventricular Failure | Acute (hours to days), can progress to Chronic HF | Reduced cardiac output, congestion (pulmonary/systemic edema), hypotension, organ hypoperfusion. Major cause of in-hospital mortality. |
| Inflammatory | Early Pericarditis, Pericardial Effusion, Dressler Syndrome | Acute (days for early pericarditis), Chronic (weeks/months for Dressler) | Chest pain (pleuritic), friction rub. Large effusions can cause tamponade. Dressler's is autoimmune. |
| Thromboembolic | Left Ventricular Mural Thrombus, Systemic Embolism (e.g., Stroke) | Subacute to Chronic (days to months) | Risk increased by large anterior MI, aneurysm, severe LV dysfunction, AF. Requires anticoagulation for prevention/treatment. |
| Structural Remodeling | LV Dilation, LV Aneurysm, Scar Formation | Chronic (weeks to years) | Leads to progressive worsening of LV function, chronic heart failure. Assessed by imaging (Echo, MRI). Target for medications (ACEi, ARBs, Beta-blockers). |
| Ischemic | Infarct Extension, Re-infarction, Post-infarction Angina | Acute to Chronic | Indicates ongoing myocardial jeopardy, requires investigation and potentially further revascularization. |
| Psychological | Depression, Anxiety, PTSD | Subacute to Chronic | Common, impacts recovery, adherence, quality of life, and potentially cardiovascular outcomes. Requires screening and management. |
Diagnosis and Management
Diagnosing post-MI sequelae relies on clinical assessment, electrocardiogram (ECG) monitoring, cardiac biomarkers, and cardiac imaging.
- Echocardiography: The mainstay for assessing overall heart function (ejection fraction), detecting wall motion abnormalities, identifying mechanical complications (rupture, VSR, PMR), evaluating valve function, and screening for pericardial effusion or LV thrombus.
- Cardiac Magnetic Resonance (CMR) Imaging: Considered the gold standard for assessing infarct size, scar tissue burden, microvascular obstruction (MO), detecting subtle structural abnormalities like thrombi or aneurysms, and evaluating ventricular remodeling. CMR parameters have significant prognostic value.
- Electrocardiogram (ECG): Used to monitor for arrhythmias, conduction blocks, signs of ongoing ischemia or re-infarction (e.g., ST-segment changes), and pericarditis.
Management focuses on treating the specific complication (e.g., emergency surgery for mechanical ruptures, antiarrhythmic drugs or devices for arrhythmias, anticoagulation for thrombus) and implementing comprehensive secondary prevention strategies. This includes lifestyle modifications (diet, exercise, smoking cessation), cardiac rehabilitation, and guideline-directed medical therapy (GDMT) with agents like beta-blockers, ACE inhibitors or ARBs, statins, antiplatelet agents, and potentially aldosterone antagonists or SGLT2 inhibitors to reduce mortality, prevent recurrent events, and mitigate adverse remodeling and heart failure progression.

Lifestyle changes are a cornerstone of secondary prevention after MI.
Understanding Complications: A Visual Guide
This video provides an educational overview of various complications that can arise after a heart attack, explaining the underlying mechanisms and clinical presentations.
The video details common issues such as arrhythmias, heart failure, structural damage like septal or papillary muscle rupture, and inflammatory responses like pericarditis, aligning with the sequelae discussed. It emphasizes the importance of recognizing these potential problems in the post-MI setting.
Frequently Asked Questions (FAQ)
What causes mechanical complications like heart rupture after an MI?
What is ventricular remodeling and why is it bad?
What is Dressler Syndrome?
Are psychological problems common after a heart attack?
Recommended Further Exploration
- What is the long-term prognosis for individuals who experience complications after a myocardial infarction?
- How does cardiac MRI help in detecting and assessing the severity of post-MI sequelae?
- What are the current management strategies for heart failure that develops after a myocardial infarction?
- What steps can be taken to prevent or minimize the risk of complications following a heart attack?
References
Last updated May 4, 2025