
Navigating Prostate Biopsies: Understanding Your Options and Results
A detailed guide to various prostate biopsy procedures, the test results that prompt them, and their respective advantages and disadvantages.
A prostate biopsy is a crucial medical procedure primarily used to diagnose prostate cancer. It involves taking small samples of tissue from the prostate gland, which are then examined under a microscope for cancerous cells. The decision to undergo a biopsy, and which type to choose, often follows initial tests that suggest potential prostate abnormalities. Understanding the different biopsy methods, what triggers their recommendation, and their pros and cons is vital for informed decision-making.
Key Insights into Prostate Biopsies
- Diverse Procedures: Several types of prostate biopsies exist, primarily differing in the approach to accessing the prostate (e.g., transrectal, transperineal) and the guidance technology used (e.g., ultrasound, MRI).
- Indications Vary: The need for a biopsy and the choice of procedure are typically guided by results such as elevated Prostate-Specific Antigen (PSA) levels, abnormal Digital Rectal Exam (DRE) findings, or suspicious areas identified on an MRI.
- Risk-Benefit Balance: Each biopsy method has a unique profile of benefits, such as higher accuracy or better sampling of certain prostate regions, and risks, including infection, bleeding, and discomfort.
When is a Prostate Biopsy Recommended?
A urologist may recommend a prostate biopsy based on several indicators suggesting the possible presence of prostate cancer. These diagnostic triggers help determine the urgency and, in some cases, the most appropriate type of biopsy.
Common Triggers for a Biopsy
Elevated Prostate-Specific Antigen (PSA) Levels
PSA is a protein produced by cells of the prostate gland. While elevated PSA levels (e.g., above 4.0 ng/mL, though this threshold can vary with age and other factors) can indicate prostate cancer, they can also be caused by non-cancerous conditions like benign prostatic hyperplasia (BPH) or prostatitis. A persistently high or rapidly rising PSA level is a common reason to proceed with a biopsy.
Abnormal Digital Rectal Exam (DRE)
During a DRE, a doctor inserts a gloved, lubricated finger into the rectum to feel the prostate for abnormalities in size, shape, or texture. The detection of hard areas, nodules, or asymmetry can be suspicious for cancer and warrant a biopsy, even if PSA levels are normal.
Suspicious MRI Findings
Multiparametric Magnetic Resonance Imaging (mpMRI) of the prostate is increasingly used before a biopsy. This advanced imaging can identify specific areas within the prostate that are suspicious for clinically significant cancer (often graded using the PI-RADS system). If an mpMRI reveals such lesions, a targeted biopsy is often recommended.
Previous Atypical or Suspicious Biopsy Results
If a prior biopsy revealed atypical cells (e.g., Atypical Small Acinar Proliferation - ASAP) or High-Grade Prostatic Intraepithelial Neoplasia (PIN), which are considered pre-cancerous or suspicious, a repeat biopsy may be recommended. This is to monitor for the development of cancer or to obtain more definitive samples.
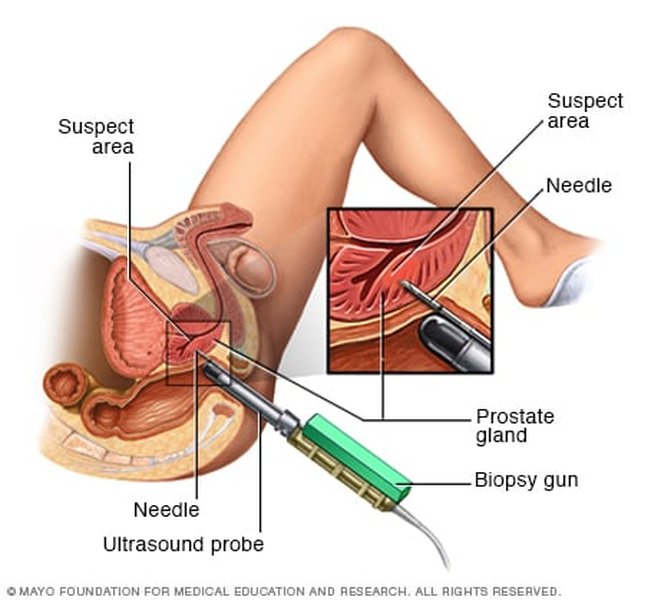
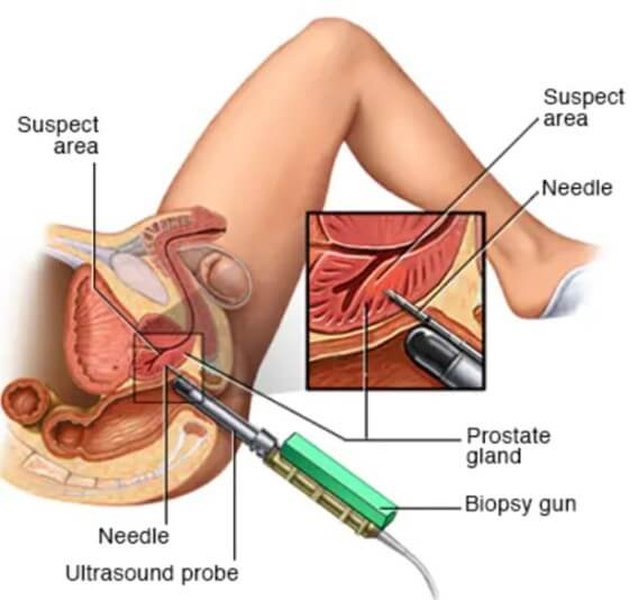
Visual representation of a prostate biopsy.
Exploring Different Types of Prostate Biopsies
Several techniques are available for performing a prostate biopsy, each with distinct methodologies, advantages, and disadvantages. The choice of procedure depends on various factors, including previous biopsy history, specific clinical indications, available technology, and patient preference.
1. Transrectal Ultrasound (TRUS)-Guided Biopsy
The Procedure
This is historically the most common method. An ultrasound probe is inserted into the rectum to create images of the prostate. A thin, spring-loaded needle is then passed through the rectal wall into the prostate to collect multiple core samples (typically 8-12, sometimes more) from different regions of the gland. Local anesthesia is usually administered.
Pros:
- Widely available and familiar to most urologists.
- Can be performed quickly in an outpatient setting or urologist's office.
- Generally well-tolerated with local anesthesia.
Cons:
- Carries a higher risk of infection (e.g., urinary tract infection, sepsis) because the needle passes through the rectal wall, which contains bacteria. Prophylactic antibiotics are typically prescribed, but antibiotic resistance is a growing concern.
- May cause temporary rectal bleeding, blood in urine (hematuria), or blood in semen (hematospermia).
- Has limitations in accessing certain parts of the prostate, particularly the anterior (front) region, potentially leading to false-negative results (missing existing cancer).
When it's often used:
Often the first-line biopsy approach when PSA levels are elevated or DRE is abnormal, especially if MRI is not readily available or indicated.
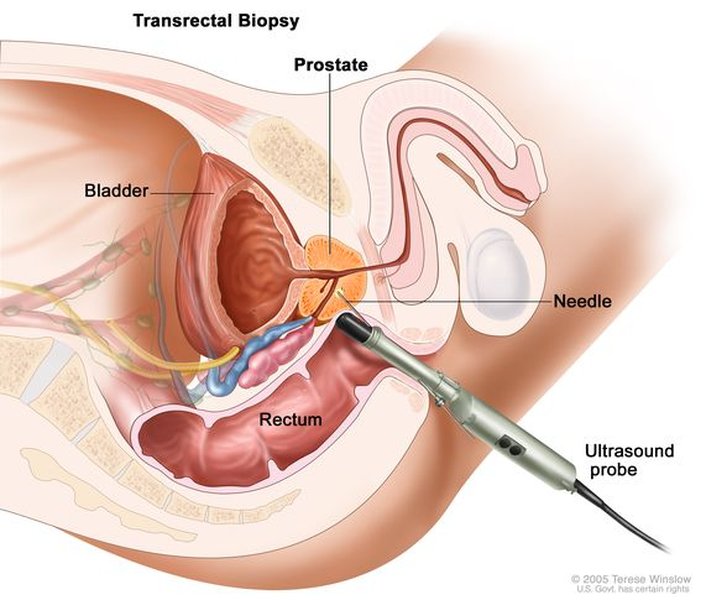
Illustration of the TRUS-guided biopsy approach.
2. Transperineal Biopsy (TPB)
The Procedure
In this method, the biopsy needle is inserted through the perineum (the skin between the scrotum and the anus) to reach the prostate. This approach avoids passing the needle through the rectal wall. TPB can be performed under local anesthesia, sedation, or general anesthesia and can be guided by ultrasound or MRI.
Pros:
- Significantly lower risk of infection compared to the TRUS approach, as the needle does not traverse the rectum. Some studies suggest infection rates near zero, potentially obviating the need for prophylactic antibiotics and helping combat antibiotic resistance.
- Provides excellent access to all areas of the prostate, including the anterior and apical regions, which can improve cancer detection rates.
- Increasingly considered a safer standard of care in many centers.
Cons:
- May cause more initial discomfort, bruising, or pain in the perineal area.
- Can sometimes lead to temporary urinary symptoms, such as difficulty urinating, if the prostate swells.
- May require more specialized training and equipment, and might be less widely available than TRUS biopsy in some regions.
- Procedure time might be slightly longer.
When it's often used:
Recommended for patients with a higher risk of infection, those who have had previous negative TRUS biopsies but still have a suspicion of cancer, or when targeting lesions identified on MRI, particularly in the anterior prostate. It is also favored when trying to reduce antibiotic use.
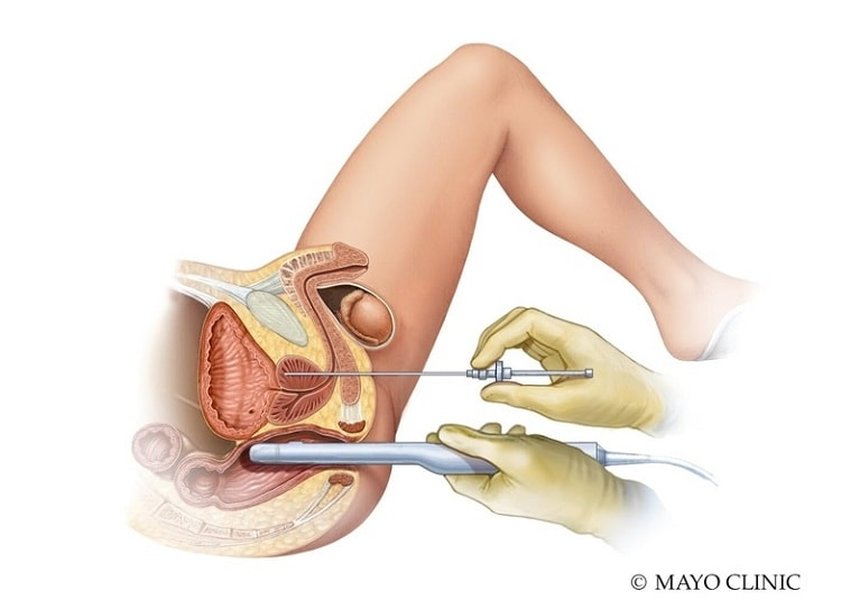
Transperineal biopsy offers a different access route to the prostate.
3. MRI-Guided Targeted Biopsy (including MRI-Ultrasound Fusion Biopsy)
The Procedure
This technique utilizes pre-biopsy mpMRI scans to identify suspicious areas within the prostate. During the biopsy, these MRI images are used to guide the needle. There are three main ways this is done:
- Cognitive Fusion: The urologist mentally fuses the MRI images with live ultrasound images.
- Software-Assisted Fusion: Specialized software overlays (fuses) stored MRI images onto live ultrasound images, providing a real-time map to target lesions.
- In-Bore MRI Biopsy: The biopsy is performed directly inside the MRI scanner, allowing for real-time MRI guidance. This is less common.
Pros:
- Increases the accuracy of detecting clinically significant prostate cancers (those more likely to be aggressive and require treatment).
- May reduce the number of cores needed compared to a standard systematic biopsy, potentially decreasing side effects.
- Can help avoid over-diagnosis of indolent (slow-growing, low-risk) cancers.
- Improves the detection of cancers in areas difficult to reach with standard TRUS biopsy.
Cons:
- Requires access to mpMRI technology and radiologists experienced in interpreting prostate MRIs.
- The fusion software and equipment can be expensive, potentially increasing the cost of the procedure.
- Availability may be limited.
- Errors in image registration or interpretation can still occur.
When it's often used:
When an mpMRI shows specific suspicious lesions (PI-RADS 3, 4, or 5), for patients with a prior negative biopsy but ongoing suspicion of cancer (e.g., rising PSA), or as an initial biopsy strategy in some centers to improve diagnostic precision.
Advanced imaging like MRI-Ultrasound fusion aids in targeting suspicious areas during a prostate biopsy.
4. Saturation Biopsy
The Procedure
A saturation biopsy involves taking a significantly larger number of core samples (often 20 or more) from the prostate than a standard biopsy. The aim is to comprehensively sample the prostate gland to reduce the chance of missing cancer.
Pros:
- May increase the cancer detection rate, especially in men with persistently elevated PSA after one or more negative standard biopsies, or in those with large prostates.
Cons:
- Higher potential for side effects such as bleeding, pain, and swelling due to the increased number of needle insertions.
- The utility and benefit over MRI-targeted approaches are debated, and it's less commonly performed now that MRI-guided techniques are more widespread.
- May increase the detection of insignificant cancers.
When it's often used:
Considered in specific situations, such as after multiple negative standard biopsies where clinical suspicion of cancer remains high, and MRI-guided options are not available or have been inconclusive.
5. Transurethral Biopsy
The Procedure
This less common method involves passing a cystoscope (a thin tube with a camera and light) through the urethra to the prostate. Tissue samples are then taken from the part of the prostate that surrounds the urethra (transition zone).
Pros:
- May be useful for diagnosing cancers located in the transition zone, which can sometimes cause urinary symptoms.
Cons:
- Not a primary method for diagnosing most prostate cancers, as they typically arise in the peripheral zone.
- Limited applicability and not widely used for initial prostate cancer screening or diagnosis.
When it's often used:
Rarely used for primary prostate cancer diagnosis; might be considered in specific cases, such as evaluating bladder outlet obstruction where transition zone cancer is suspected.
Comparative Analysis of Biopsy Techniques
To better visualize the differences, the following chart compares key aspects of the most common prostate biopsy procedures based on factors like accuracy, risk of infection, patient comfort, accessibility, and ability to sample various prostate zones. The scoring is a qualitative assessment (1-Low/Poor, 5-High/Excellent).
This radar chart illustrates a qualitative comparison of different prostate biopsy techniques. For instance, Transperineal Biopsy generally scores higher on 'Low Infection Risk' and 'Anterior Zone Access' compared to traditional TRUS. MRI-Guided Biopsy excels in 'Detection Accuracy' for significant cancers but might be lower in 'Accessibility/Cost-Effectiveness' for some. These are general trends and individual experiences or specific clinical contexts can vary.
Decision Pathway for Prostate Biopsy
The following mindmap illustrates a simplified decision-making pathway, starting from initial clinical suspicion (e.g., elevated PSA, abnormal DRE) to the selection of a particular prostate biopsy procedure. Factors like MRI findings and risk assessment play crucial roles in this pathway.
(Elevated PSA, Abnormal DRE)"] id1["Risk Assessment
& Patient Factors"] id1a["Low Infection Risk Preference"] id1b["Previous Negative Biopsies"] id1c["Prostate Size/Anatomy"] id2["Consider mpMRI"] id2a["No Suspicious Lesions on MRI"] id2a1["Systematic Biopsy (TRUS or Transperineal)"] id2b["Suspicious Lesions (PI-RADS ≥3) on MRI"] id2b1["MRI-Targeted Biopsy
(Fusion or In-Bore)"] id2b1a["+ Systematic Cores"] id2b1b["Transperineal Approach Favored"] id2b1c["Transrectal Approach (if TP not feasible)"] id3["No MRI or MRI Contraindicated"] id3a["Standard TRUS-Guided Systematic Biopsy"] id3b["Transperineal Systematic Biopsy
(if infection risk is high or preferred)"] id4["High Suspicion despite Negative Biopsies"] id4a["Repeat Biopsy with MRI-Guidance"] id4b["Consider Saturation Biopsy (less common)"]
This mindmap outlines how initial findings like an elevated PSA or an abnormal DRE lead to further evaluation, often including an mpMRI. The results of the MRI can then guide whether a standard systematic biopsy or a more targeted MRI-guided biopsy is performed, with the transperineal approach often favored for its lower infection risk.
Summary of Pros and Cons
The choice of a prostate biopsy procedure involves weighing the benefits against the potential drawbacks. Here's a table summarizing these aspects for the main techniques:
| Biopsy Method | Pros | Cons |
|---|---|---|
| Transrectal Ultrasound (TRUS)-Guided Biopsy | Widely available; quick outpatient procedure; familiar technique. | Higher infection risk; potential for rectal bleeding; may miss anterior tumors; antibiotic resistance concerns. |
| Transperineal Biopsy (TPB) | Significantly lower infection risk (may not require antibiotics); better access to all prostate zones, including anterior; increasingly recommended. | May cause more perineal discomfort/bruising initially; can cause temporary urinary issues; may require more training/specialized setup. |
| MRI-Guided Targeted Biopsy (Fusion or In-Bore) | Higher accuracy for clinically significant cancers; better risk stratification; may reduce number of cores and over-diagnosis of indolent cancer. | Requires MRI availability and expertise; higher cost; more complex procedure; still carries risks of access route (TRUS or TPB). |
| Saturation Biopsy | May increase detection if prior biopsies were negative despite high suspicion. | Increased risk of side effects; less commonly used with advent of MRI-guidance; may detect more insignificant cancers. |
| Transurethral Biopsy | Can sample transition zone if specific suspicion exists. | Limited applicability for most prostate cancers (which are peripheral); not a standard diagnostic tool for initial assessment. |
Understanding Your Pathology Report
After the biopsy, tissue samples are sent to a pathologist. Key findings in the report include:
- Presence of Cancer: Whether cancer cells (typically adenocarcinoma) are found.
- Gleason Score: If cancer is present, this score (ranging from 6 to 10) grades its aggressiveness based on how abnormal the cells appear. A score of 6 is low-grade, 7 is intermediate-grade, and 8-10 are high-grade. This is often reported as Grade Groups 1 through 5.
- Number of Positive Cores: How many samples contain cancer.
- Percentage of Cancer in Each Core: The extent of cancer within each positive sample.
- Perineural Invasion: Whether cancer cells are seen growing along nerves.
- Atypical Findings: Presence of High-Grade PIN or ASAP, which may warrant further monitoring or repeat biopsy.
Understanding these results is crucial for determining the next steps, whether it's active surveillance, treatment, or further diagnostic tests.
This video provides an overview of what to expect from a prostate biopsy procedure, which can be helpful for patients preparing for this diagnostic test.
Frequently Asked Questions (FAQ)
Conclusion
Prostate biopsy is the definitive method for diagnosing prostate cancer. The evolution of biopsy techniques, particularly the increasing use of mpMRI guidance and the transperineal approach, aims to improve diagnostic accuracy while minimizing risks, especially infection. Understanding the various types of procedures, why one might be recommended over another based on your specific test results and risk factors, and the potential pros and cons of each, empowers you to have informed discussions with your healthcare provider and make decisions that are best suited to your individual situation.
Recommended Further Insights
- What does the Gleason score mean in my prostate biopsy report?
- How does multiparametric MRI improve prostate cancer detection before a biopsy?
- What are the long-term implications of High-Grade PIN found on a prostate biopsy?
- Comparing active surveillance versus immediate treatment for low-grade prostate cancer.
References
Last updated May 21, 2025