
Unraveling the Puzzle: How a Single Bone Metastasis Can Emerge with Seemingly Localized Prostate Cancer
Exploring the advanced imaging and biological factors that can lead to unexpected metastatic findings in your specific case.
It's understandable to question how a single bone metastasis could be detected when other indicators suggest your prostate cancer is localized. Your PSA level of 9.3 ng/mL, PSA density of 0.07 ng/mL², Gleason scores of 6 and 7, and normal findings in your lymph nodes and seminal vesicles indeed paint a picture often associated with cancer confined to the prostate. However, the discovery of a single focal sclerotic metastasis in your left ischial tuberosity via PSMA PET/CT, with a high SUVmax of 16.59, reveals a more complex situation. Let's delve into the factors that can explain this scenario.
Key Insights into Your Situation
- The Power of PSMA PET/CT: This advanced imaging is highly sensitive and can detect small, isolated cancer deposits that older imaging techniques might miss. Your high SUVmax value (16.59) strongly indicates active cancer cells at that specific bone site.
- Prostate Cancer's Affinity for Bone: Prostate cancer cells have a known tendency to travel to and grow in bones. This can happen even when the primary tumor seems contained.
- Early Microscopic Spread: Cancer cells can detach from the main tumor and enter the bloodstream or lymphatic system early in the disease process, sometimes establishing a distant outpost like a single bone metastasis before widespread disease is evident.
Understanding Your Clinical Profile
Your clinical parameters provide important clues, but they don't always tell the whole story. Here's a breakdown:
Prostate-Specific Antigen (PSA) and PSA Density
PSA Level: 9.3 ng/mL
A PSA of 9.3 ng/mL is elevated above the typical normal range but is not exceptionally high. It can be associated with localized prostate cancer, but it's not a definitive indicator of whether the cancer has spread. Some tumors can metastasize even with moderate PSA levels.
PSA Density: 0.07 ng/mL²
Your PSA density (PSA level divided by prostate volume) of 0.07 is relatively low. A lower PSA density often suggests a lower likelihood of aggressive cancer or that the elevated PSA might be partly due to benign prostatic hyperplasia (BPH). However, like PSA itself, PSA density is not a perfect predictor of metastatic risk, and some tumor cells can still behave aggressively and spread despite a low overall density.
Gleason Score: 6 and 7
Your biopsy revealed prostate cancer with Gleason scores of 6 and 7. This is significant:
- Gleason 6 (e.g., 3+3): This is considered low-grade cancer. It typically grows slowly and has a very low potential to metastasize. Studies show that pure Gleason 6 cancer rarely spreads.
- Gleason 7 (e.g., 3+4 or 4+3): This is intermediate-risk cancer. The presence of pattern 4 cells (either as 3+4=7 or 4+3=7) indicates a more aggressive potential than Gleason 6. Gleason 7 cancers have a notably higher chance of growing and spreading outside the prostate compared to Gleason 6. The Gleason 7 component in your cancer is a key factor that could contribute to the possibility of metastasis, even if it's a single site.
Localized Disease and Normal Regional Findings
The assessment that your cancer is "localized in the prostate gland" with "normal lymph nodes and seminal vesicles" is based on initial imaging (likely MRI or CT). This suggests no visible spread to the areas immediately surrounding the prostate. However, these conventional imaging techniques may not detect microscopic cancer cells that have already traveled to distant sites like bone.
Explaining the Single Bone Metastasis
Several interconnected factors explain how a single bone metastasis can be present in your left ischial tuberosity (a part of your pelvis) despite the other findings:
1. The "Seed and Soil" Hypothesis and Bone Tropism
Prostate cancer has a well-documented predilection for bone. This is often explained by the "seed and soil" theory:
- The "Seeds": Cancer cells from the prostate tumor can detach and enter the bloodstream.
- The "Soil": Bones, particularly areas rich in red marrow like the pelvis (including the ischial tuberosity), spine, and ribs, provide a fertile "soil" or microenvironment conducive to the survival and growth of these prostate cancer "seeds." This hospitable environment is due to various growth factors and cellular interactions within the bone.

Conceptual illustration of prostate cancer cells metastasizing to bone.
2. Early Microscopic Dissemination
Cancer cells can spread from the primary tumor early in the disease, even when the tumor appears small and confined to the prostate. These microscopic clusters of cells, or even single cells, can travel through the bloodstream and lie dormant in a distant site like bone for some time before growing into a detectable metastasis. Your single lesion could represent such an early event.
3. The High Sensitivity of PSMA PET/CT with F-18
What is PSMA PET/CT?
Prostate-Specific Membrane Antigen (PSMA) is a protein found at high levels on the surface of most prostate cancer cells. PSMA PET/CT uses a radioactive tracer (in your case, labeled with F-18) that binds specifically to PSMA. This allows the PET scanner to light up areas where prostate cancer cells are present, anywhere in the body.
Why is it significant in your case?
PSMA PET/CT is significantly more sensitive than traditional imaging modalities like conventional bone scans or CT scans for detecting prostate cancer spread, especially small volume or early metastatic disease. It can identify lesions that other scans might miss. The "focal" nature of your lesion means it's a distinct, localized spot of uptake.
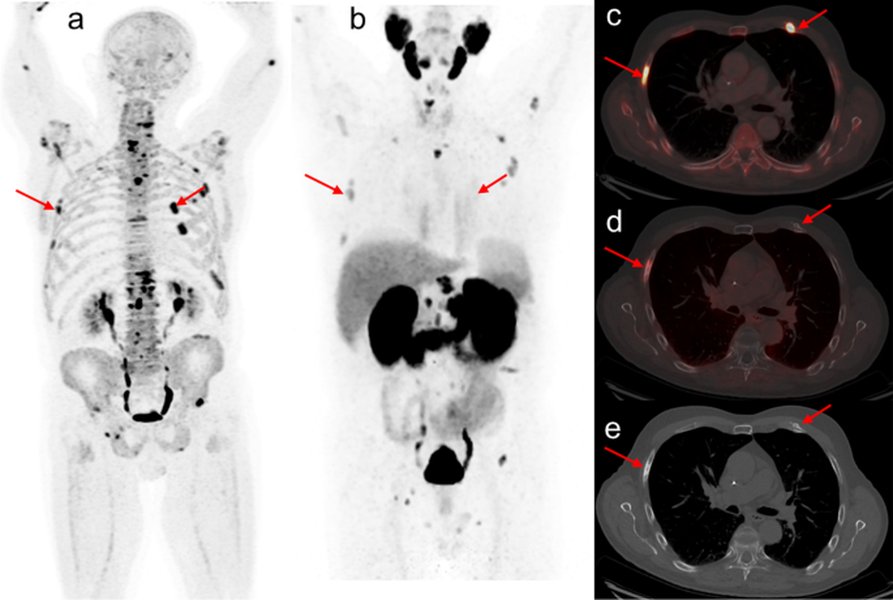
Example image showing how PSMA PET/CT can highlight areas of prostate cancer activity.
SUVmax of 16.59
The Standardized Uptake Value (SUVmax) measures the intensity of tracer uptake in a lesion. An SUVmax of 16.59 is considered high, indicating significant metabolic activity and a high concentration of PSMA-expressing cells. This high value strongly suggests that the lesion in your ischial tuberosity is indeed a prostate cancer metastasis rather than a benign bone lesion, although very rarely other conditions can cause PSMA uptake.
4. The Concept of Oligometastatic Disease
Oligometastasis refers to a state where a patient has a limited number of metastatic lesions (typically 1 to 5) at a few sites. This is an increasingly recognized stage of cancer. It's possible that your cancer has spread, but only to this single site so far. The detection of such limited disease is often thanks to advanced imaging like PSMA PET/CT. This finding is crucial as it changes the cancer stage and may open up different treatment considerations, potentially including targeted therapy to the metastasis alongside treatment for the primary prostate cancer.
5. Tumor Heterogeneity
Prostate tumors are often heterogeneous, meaning they can be composed of different types of cancer cells with varying degrees of aggressiveness. While your biopsy showed Gleason 6 and 7 patterns, it's possible that a small, more aggressive component within the tumor (perhaps not fully represented in the biopsy samples) was responsible for shedding cells that led to this metastasis.
6. Stochastic (Random) Element of Metastasis
The process of metastasis involves a complex cascade of events, and there's an element of chance involved in whether a circulating tumor cell will successfully establish a new tumor at a distant site. It's conceivable that, by chance, only one such event has successfully occurred and become detectable at this point.
Summary of Clinical Findings and Implications
The following table summarizes your key clinical findings and their relevance to the detection of a single bone metastasis:
| Clinical Finding | Your Value/Observation | Typical Implication for Localized Disease | Relevance to Your Single Metastasis |
|---|---|---|---|
| PSA Level | 9.3 ng/mL | Elevated, but can be consistent with localized cancer. | Not a perfect predictor of spread; metastasis can occur even with moderate PSA levels. |
| PSA Density | 0.07 ng/mL² | Relatively low; often suggests less aggressive local disease or less cancer volume relative to prostate size. | Does not rule out the metastatic potential of specific cancer cell clones within the tumor. |
| Gleason Score | 6 and 7 | A mix of low-grade (Gleason 6) and intermediate-grade (Gleason 7) cancer. | The Gleason 7 component (especially if pattern 4 is present) significantly increases the potential for metastasis compared to Gleason 6 alone. |
| Primary Tumor Status | Localized in prostate gland (by initial imaging) | Cancer appears confined to the prostate. | Microscopic cells may have already escaped the prostate and traveled to distant sites before this assessment. |
| Lymph Nodes & Seminal Vesicles | Normal (by initial imaging) | No evidence of spread to nearby structures. | Distant metastasis (like to bone) can sometimes occur without prior or concurrent detectable spread to regional lymph nodes. |
| PSMA PET/CT Finding | Single focal sclerotic lesion in left ischial tuberosity | N/A (This is the metastatic finding) | Highly sensitive PSMA PET/CT detected a specific bone lesion characteristic of prostate cancer, appearing dense (sclerotic). |
| PSMA PET/CT SUVmax | 16.59 | N/A | Very high tracer uptake strongly indicates metabolically active prostate cancer cells, confirming the lesion's malignant nature. |
Visualizing Contributing Factors: Metastasis Detection Profile
The radar chart below illustrates a conceptual profile of factors that can contribute to the detection of metastasis in a scenario like yours. The scores are illustrative, on a scale of 1 (low influence/value) to 10 (high influence/value), reflecting how each factor might play a role. For instance, "Imaging Sensitivity" is high due to the PSMA PET/CT, while "PSA Level as Sole Predictor" might be rated lower because PSA alone isn't definitive.
This chart visually represents how factors like the high sensitivity of PSMA PET imaging and the inherent bone tropism of prostate cancer can lead to the detection of a metastasis, even when some other indicators (like PSA density) might seem less alarming.
How Prostate Cancer Metastasizes to Bone
The video below provides a general overview of how prostate cancer can spread to the bones, discussing the biological mechanisms involved. Understanding this process can further clarify why bone is a common site for metastases.
This video explains the "vicious cycle" where cancer cells interact with bone cells (osteoblasts and osteoclasts), leading to changes in bone structure – in your case, sclerotic (bone-forming) changes.
Mapping the Factors: A Mindmap View
This mindmap provides a visual summary of the key elements involved in understanding your specific situation: your clinical profile, the details of the metastatic lesion, and the primary reasons explaining its occurrence despite other seemingly localized features.
Detects small/early lesions"] id3b["Prostate Cancer's Natural Affinity for Bone (Tropism)
'Seed and Soil' Hypothesis"] id3c["Early Microscopic Dissemination of Cancer Cells
Spread before detection of widespread disease"] id3d["Metastatic Potential of Gleason 7 Component
Pattern 4 cells increase risk"] id3e["Concept of Oligometastatic Disease
Limited number of metastases (in this case, one)"] id3f["Possible Tumor Heterogeneity
Undetected aggressive cell clones"] id4["Reconciling the Findings"] id4a["Limitations of PSA/PSA Density as Sole Predictors of Spread"] id4b["Conventional Imaging (for primary tumor) vs. Advanced Molecular Imaging (PSMA PET)"] id4c["Stochastic Nature of Metastatic Process"]
This mindmap illustrates how the high sensitivity of PSMA PET/CT, combined with the biological characteristics of prostate cancer (like bone tropism and the influence of the Gleason 7 component), can lead to the identification of a solitary bone metastasis even when other initial findings suggest localized disease.
Frequently Asked Questions (FAQ)
Recommended Further Exploration
To deepen your understanding, you might find these related queries helpful:
- What are the current treatment options for oligometastatic prostate cancer?
- How are PSMA PET CT SUVmax values interpreted in diagnosing prostate cancer metastases?
- What is the role of Gleason score 7 in prostate cancer prognosis and its likelihood of spreading?
- How can bone health be managed when prostate cancer has spread to the bones?
References
Last updated May 7, 2025