
Unlocking the Mystery of Radiculopathy: When Nerve Roots Cry Out
A deep dive into the causes, symptoms, and treatments for that "pinched nerve" feeling.
Radiculopathy is a term you might hear if you're experiencing pain, numbness, or weakness that seems to travel from your spine into your limbs. Often described as a "pinched nerve," this condition arises when a nerve root in your spinal column becomes compressed or irritated. Understanding radiculopathy is the first step towards finding relief and improving your quality of life. This comprehensive guide will explore what radiculopathy is, its various types, common causes, tell-tale symptoms, how it's diagnosed, and the available treatment options.
Quick Insights: Key Takeaways on Radiculopathy
- Nerve Root Compression: Radiculopathy fundamentally involves the compression or irritation of a spinal nerve root, which is where a nerve branches off from the spinal cord.
- Radiating Symptoms: The hallmark symptoms include pain, numbness, tingling, and weakness that radiate along the path of the affected nerve, often into an arm or leg.
- Varied Causes & Locations: It can occur in the neck (cervical), lower back (lumbar), or mid-back (thoracic) and is commonly caused by conditions like herniated discs or spinal stenosis.
What Exactly Is Radiculopathy?
Radiculopathy refers to a range of symptoms produced by the pinching or irritation of a nerve root as it exits the spinal column. The term itself combines "radix" (Latin for root) and "pathos" (Ancient Greek for suffering), literally meaning a problem at the nerve root. These nerve roots are crucial as they transmit signals between your spinal cord and the rest of your body, controlling sensation and muscle movement.
The Spine's Anatomy and Nerve Pathways
To understand radiculopathy, it's helpful to know a bit about your spine. It's made up of individual bones called vertebrae, stacked one on top of another. Between these vertebrae are intervertebral discs, which act as cushions and allow for flexibility. The spinal cord runs through a central canal within the vertebrae. Nerve roots branch off from the spinal cord at each vertebral level, exiting through small openings called foramina. Radiculopathy occurs when these nerve roots are compressed or inflamed at or near these foramina.

Illustration showing cervical nerve roots and potential points of compression.
Types of Radiculopathy: Location Matters
Radiculopathy is classified based on where along the spine the nerve compression occurs:
-
Cervical Radiculopathy
This type affects the nerve roots in the neck (cervical spine). It's less common than lumbar radiculopathy, with an estimated prevalence of about 83 cases per 100,000 people in the USA. Symptoms typically include pain, numbness, or weakness that radiates from the neck into the shoulders, arms, or hands. The C7 and C6 nerve roots are most commonly affected. Risk factors include being aged 40-50, female gender, white race, and cigarette smoking. Poor posture and certain high-impact activities can exacerbate symptoms.
-
Lumbar Radiculopathy
This is the most frequently diagnosed type, affecting the nerve roots in the lower back (lumbosacral region). Its prevalence is estimated to be 3-5% of the population. Symptoms include pain, tingling, or weakness that often starts in the lower back and radiates down through the hips, buttocks, and into one or both legs. This is commonly referred to as "sciatica" when the sciatic nerve (formed by nerve roots L4-S3) is involved. The L4-L5 and L5-S1 levels are most susceptible, accounting for about 90% of cases. Age is a primary risk factor, with men often affected in their 40s and women in their 50s and 60s.
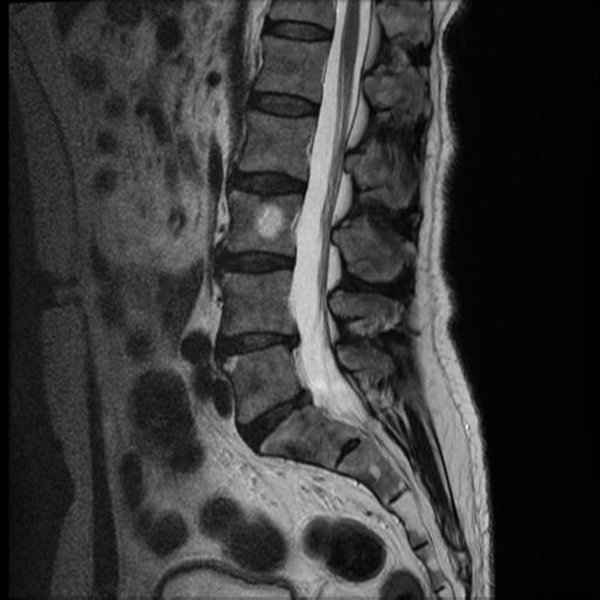
MRI demonstrating a lumbar disc protrusion impinging on a nerve root.
-
Thoracic Radiculopathy
This is the least common type, involving a compressed nerve root in the upper or mid-back (thoracic spine). Symptoms often manifest as pain and numbness that wrap around the front of the body in a band-like pattern, sometimes mistaken for conditions like shingles. Weakness in the muscles controlled by the affected thoracic nerves can occur but is less common.
Unmasking the Culprits: Common Causes of Radiculopathy
Radiculopathy is most often caused by mechanical compression or inflammation of a nerve root due to changes in the tissues surrounding it. Key culprits include:
- Herniated or Bulging Disc: Spinal discs can weaken, bulge, or rupture (herniate), allowing the inner gel-like material to press against a nearby nerve root. This is a very common cause, implicated in about 21.9% of radiculopathy cases.
- Spondylosis (Degenerative Disc Disease/Osteoarthritis): Age-related wear and tear can lead to degeneration of the discs and facet joints in the spine. This can result in the formation of bone spurs (osteophytes) that narrow the foramina, a condition known as foraminal stenosis.
- Spinal Stenosis: This refers to a general narrowing of the spinal canal or the foraminal openings, which can put pressure on the spinal cord or nerve roots.
- Thickening (Ossification) of Spinal Ligaments: Ligaments in the spine can thicken and harden over time, reducing space for the nerve roots.
- Spondylolisthesis: This condition occurs when one vertebra slips forward over the vertebra below it, potentially pinching nerve roots.
- Less Common Causes: Other, less frequent causes include spinal infections (e.g., shingles, Lyme disease, HIV), cancerous or non-cancerous growths (tumors) in the spine, spinal epidural abscess or hematoma, trauma or injury to the spine, proximal diabetic neuropathy causing nerve ischemia, Tarlov cysts, sarcoidosis, and arachnoiditis.

An MRI scan illustrating features consistent with cervical radiculopathy, such as disc herniation or foraminal stenosis.
Recognizing the Signs: Symptoms of Radiculopathy
Symptoms of radiculopathy vary depending on which nerve root is affected and the severity of the compression. However, some common signs include:
- Pain: This is often the most prominent symptom. It can be sharp, shooting, burning, or aching. The pain typically radiates along the path of the affected nerve – for example, down an arm in cervical radiculopathy or down a leg in lumbar radiculopathy.
- Numbness: A loss of sensation or a "dead" feeling in the area supplied by the compressed nerve.
- Tingling (Paresthesia): A "pins-and-needles" sensation.
- Weakness: Difficulty moving or controlling muscles in the affected limb. This may manifest as a weakened grip, foot drop, or difficulty with coordination. Muscle strength is often affected only in more severe cases.
- Altered Reflexes: Deep tendon reflexes corresponding to the affected nerve root may be diminished or absent.
- Sensory Changes: There might be hypersensitivity to touch in some areas or a decreased ability to sense touch, temperature, or vibration.
It's important to note that radiculopathy symptoms can sometimes overlap with those of peripheral neuropathy (damage to nerves outside the spinal cord, like carpal tunnel syndrome), making an accurate diagnosis crucial.
Visualizing Symptom Profiles: A Comparative Look
The intensity and combination of symptoms like pain, numbness, tingling, and weakness can vary significantly between cervical, lumbar, and thoracic radiculopathy. The following chart provides an illustrative comparison of how these symptoms might typically present across the different types. Please note this is a generalized representation and individual experiences can differ.
This chart helps visualize how, for example, radiating pain might be a very prominent feature in lumbar radiculopathy, while muscle weakness might be comparatively less pronounced in thoracic radiculopathy. Each point represents a typical severity score out of 10.
Diagnosing Radiculopathy: Finding the Source
An accurate diagnosis is key to effective treatment. This typically involves a multi-step approach:
- Medical History and Physical Examination: Your doctor will ask about your symptoms, their onset, what makes them better or worse, and any relevant medical history. A physical exam will assess your posture, range of motion, muscle strength, sensation, and reflexes.
-
Provocative Maneuvers
Specific physical tests can help pinpoint the affected nerve root by reproducing or exacerbating your symptoms. Examples include:
- Spurling's Test: For cervical radiculopathy, this involves gently extending and rotating the neck to the affected side and applying downward pressure.
- Straight Leg Raise (SLR) Test: For lumbar radiculopathy, lifting the straightened leg while lying down can stretch the sciatic nerve and reproduce pain.
- Femoral Nerve Stretch Test: Also for lumbar issues, this test can indicate compression of higher lumbar nerve roots.
-
Imaging Tests
These help visualize the structures of the spine and identify the cause of nerve compression:
- X-rays (Projectional Radiography): Often an initial study, X-rays can show bone spurs, narrowing of disc spaces, fractures, or spinal alignment issues.
- Magnetic Resonance Imaging (MRI): MRI provides detailed images of soft tissues, including discs, nerves, and ligaments. It is excellent for identifying herniated discs, spinal stenosis, and tumors. It's important to correlate MRI findings with clinical symptoms, as disc herniations can be present in asymptomatic individuals.
- Computed Tomography (CT) Scan: CT scans provide more detailed images of bony structures than X-rays and can be useful for identifying bone spurs or foraminal stenosis.
- CT Myelogram: This involves injecting contrast dye into the spinal canal before a CT scan to highlight the spinal cord and nerve roots, useful if MRI is contraindicated or inconclusive.
-
Electrodiagnostic Testing
These tests assess nerve function:
- Electromyography (EMG): Small needles are inserted into muscles to measure their electrical activity at rest and during contraction. EMG can help confirm nerve root damage (radiculopathy) and differentiate it from peripheral neuropathy or muscle disorders. It can reveal active denervation in acute cases or neurogenic changes in chronic ones.
- Nerve Conduction Studies (NCS): These measure how quickly electrical signals travel along a nerve, helping to identify nerve damage or compression.
- Cerebrospinal Fluid Analysis: Rarely, if an infection or neoplastic cause is suspected and imaging is inconclusive, a sample of cerebrospinal fluid may be analyzed.
Mapping Radiculopathy: Core Concepts
The following mindmap provides a visual summary of the key aspects of radiculopathy, from its definition and types to its causes, symptoms, diagnosis, and treatment pathways. This can help in understanding the multifaceted nature of the condition.
Nerve root compression or irritation
leading to pain, numbness, weakness"] id2["Types"] id2a["Cervical (Neck)
Symptoms in arm/hand"] id2b["Lumbar (Lower Back)
Symptoms in leg/foot (Sciatica)"] id2c["Thoracic (Mid-Back)
Band-like pain around torso"] id3["Common Causes"] id3a["Herniated Disc"] id3b["Spondylosis (Degeneration/Arthritis)"] id3c["Spinal Stenosis (Narrowing)"] id3d["Bone Spurs (Osteophytes)"] id3e["Spondylolisthesis (Vertebral Slip)"] id3f["Ligament Thickening"] id4["Symptoms"] id4a["Radiating Pain"] id4b["Numbness"] id4c["Tingling (Paresthesia)"] id4d["Muscle Weakness"] id4e["Altered Reflexes"] id5["Diagnosis"] id5a["Medical History & Physical Exam"] id5b["Provocative Tests (Spurling's, SLR)"] id5c["Imaging (MRI, CT, X-ray)"] id5d["Electrodiagnostics (EMG/NCS)"] id6["Treatment"] id6a["Conservative (Non-Surgical)"] id6a1["Medications (NSAIDs, Analgesics)"] id6a2["Physical Therapy & Exercise"] id6a3["Epidural Steroid Injections"] id6a4["Activity Modification"] id6b["Surgical Intervention"] id6b1["Discectomy"] id6b2["Laminectomy/Foraminotomy"] id6b3["Spinal Fusion (less common for isolated radiculopathy)"]
This mindmap illustrates the interconnected elements involved in understanding and managing radiculopathy, highlighting the journey from initial symptoms to potential treatment pathways.
Treatment Pathways for Radiculopathy
The primary goals of radiculopathy treatment are to alleviate pain, restore function, and address the underlying cause of nerve compression. Most patients (over 85% for cervical radiculopathy) respond well to conservative, non-surgical treatments, often finding relief within 8 to 12 weeks.
Non-Surgical (Conservative) Management
This is typically the first line of approach:
- Medications:
- Nonsteroidal Anti-Inflammatory Drugs (NSAIDs): Medications like ibuprofen or naproxen can help reduce pain and inflammation.
- Oral Corticosteroids: A short course might be prescribed to reduce severe inflammation.
- Muscle Relaxants: Can help alleviate muscle spasms accompanying the pain.
- Neuropathic Pain Medications: Drugs like gabapentin or pregabalin may be used for chronic nerve pain.
- Opioid Analgesics: Used cautiously for short-term management of severe pain due to potential for dependence.
- Physical Therapy: A cornerstone of conservative treatment. Therapists design individualized programs that may include:
- Exercises to strengthen core and spinal muscles.
- Stretching exercises to improve flexibility and relieve pressure.
- Postural education and ergonomic advice.
- Manual therapy techniques.
- Mechanical traction, especially for cervical radiculopathy, combined with exercise, has shown positive long-term effects.
- Epidural Steroid Injections: Corticosteroid medication is injected directly into the epidural space around the affected nerve root, often under X-ray guidance (fluoroscopy). This can provide significant short-term pain relief by reducing inflammation, allowing patients to participate more effectively in physical therapy.
- Activity Modification: Avoiding activities or positions that worsen symptoms, such as heavy lifting, prolonged sitting or standing in poor posture, or specific movements (e.g., tilting head to the side of a pinched nerve in cervical radiculopathy).
- Lifestyle Modifications: Weight management, smoking cessation (as smoking can impair healing and disc health), and adopting healthy habits.
This video provides a patient-friendly overview of radiculopathy, explaining what it is and common symptoms.
The embedded video offers a general educational insight into radiculopathy, discussing its nature as a condition arising from spinal nerve compression or irritation. It briefly touches upon the resulting symptoms such as pain, numbness, and weakness, which aligns with the comprehensive information provided in this guide. Such educational resources can be helpful for patients to grasp the basic concepts of their condition.
Surgical Intervention
Surgery may be considered if:
- Conservative treatments fail to provide adequate relief after an extended period (e.g., 6-12 weeks).
- There is progressive neurological deficit, such as increasing muscle weakness.
- Symptoms are severe and significantly impacting quality of life.
- There are signs of severe nerve compression or conditions like cauda equina syndrome (a medical emergency involving compression of nerve roots at the very end of the spinal cord, causing symptoms like bowel/bladder incontinence, severe leg weakness, or saddle anesthesia), which requires urgent surgical decompression.
- Discectomy (or Microdiscectomy): Removal of the portion of a herniated disc that is pressing on the nerve root.
- Laminectomy/Laminotomy: Removal of a small portion of the lamina (the bony arch of a vertebra) to create more space for the nerve root.
- Foraminotomy: Enlarging the foramen (the opening where the nerve root exits the spine).
- Spinal Fusion: In some cases, particularly if there's instability or significant degenerative changes, vertebrae may be fused together after decompression. This is less common for isolated radiculopathy without instability.
The choice of treatment depends on the specific cause, location, severity of symptoms, and individual patient factors. A multidisciplinary team, including spine specialists, physicians, and therapists, often collaborates to provide the best care.
Comparing Radiculopathy Types: A Quick Overview
The following table summarizes key distinguishing features of cervical, lumbar, and thoracic radiculopathy, offering a comparative perspective that can aid in understanding the nuances of each type.
| Feature | Cervical Radiculopathy | Lumbar Radiculopathy | Thoracic Radiculopathy |
|---|---|---|---|
| Location of Symptoms | Neck, shoulder, arm, hand, fingers | Lower back, buttock, hip, leg, foot | Mid-back, chest, abdomen (band-like) |
| Common Nerve Roots Affected | C5, C6, C7 (most common), C8 | L4, L5, S1 (most common) | T1-T12 (variable, less common) |
| Typical Pain Pattern | Radiating pain, often sharp or burning, from neck down the arm | Radiating pain (sciatica), often sharp, shooting, or aching, from low back down the leg | Burning or shooting pain wrapping around the torso |
| Common Causes | Disc herniation, spondylosis (foraminal stenosis, bone spurs) | Disc herniation, spondylosis (foraminal stenosis, bone spurs), spinal stenosis | Disc herniation (less common here), spondylosis, trauma, diabetes |
| Prevalence | Less common than lumbar (approx. 83/100,000) | Most common (approx. 3-5% of population) | Least common |
| Associated Weakness Examples | Deltoid (C5), Biceps/Wrist Extensors (C6), Triceps/Wrist Flexors (C7), Hand intrinsics (C8/T1) | Quadriceps/Ankle Dorsiflexion (L4), Great Toe Extension (L5), Ankle Plantarflexion (S1) | Intercostal muscles, abdominal wall muscles (rarely significant) |
This table provides a snapshot of how radiculopathy manifests differently depending on the spinal region affected, emphasizing the importance of precise diagnosis for targeted treatment.
Prognosis and Outlook
The prognosis for radiculopathy is generally favorable. Most individuals experience significant improvement with conservative treatments over a period of weeks to months. For instance, over 85% of patients with acute cervical radiculopathy find relief within 8-12 weeks with non-surgical care. Early diagnosis and appropriate, targeted treatment are crucial for pain relief and preventing chronic issues. Even if symptoms persist, many management strategies can help maintain a good quality of life. A multidisciplinary approach involving physicians, physical therapists, and sometimes pain management specialists can be very effective.
Frequently Asked Questions (FAQ)
Conclusion
Radiculopathy, essentially a "pinched nerve" in the spine, is a common condition that can cause significant discomfort through radiating pain, numbness, tingling, and weakness. It arises from various causes, most frequently herniated discs and degenerative changes in the spine affecting the cervical, lumbar, or thoracic regions. A thorough diagnostic process involving clinical examination and imaging is crucial for pinpointing the affected nerve root and its cause. Fortunately, a majority of individuals find relief through conservative treatments like medication, physical therapy, and lifestyle adjustments. When these measures are insufficient, or if neurological deficits are progressive, surgical options can provide effective decompression and symptom resolution. Understanding the nature of radiculopathy empowers individuals to seek timely and appropriate care, leading to better outcomes and an improved quality of life.
Recommended Further Exploration
- What are the best physical therapy exercises for lumbar radiculopathy?
- How does spinal stenosis cause cervical radiculopathy?
- When is surgery recommended for a herniated disc causing radiculopathy?
- Can lifestyle changes like diet and posture help prevent radiculopathy?
References
Last updated May 21, 2025